
Managing recurrent depression and persistent anxiety often feels like an endless cycle of trial and error. While traditional psychotherapy and medication management serve as vital foundational tools, many individuals actively seek holistic, evidence-based practices to maintain their long-term mental wellbeing.
This is where Mindfulness-Based Cognitive Therapy (MBCT) enters the conversation.
If you are exploring MBCT for depression and anxiety, understanding what the clinical data actually proves can help you make an informed choice. Below, we break down the latest meta-analyses, analyze clinical effect sizes, and explore how this integrative approach fits into a comprehensive, whole-person psychiatric care plan.
MBCT for Depression & Anxiety: Key Research Numbers at a Glance
Before diving into the detailed clinical trials, here is a quick summary of what the pooled scientific research shows about the efficacy of Mindfulness-Based Cognitive Therapy:
-
Symptom Relief: MBCT provides modest, reliable drops in acute anxiety and depression symptoms compared to waitlist or standard treatment-as-usual (TAU).
-
Relapse Prevention: This is where MBCT truly shines. Clinical evidence proves it significantly lowers the risk of depressive relapse, performing on par with maintenance antidepressant medication.
-
Long-Term Durability: Follow-up data indicates that the psychological gains and coping mechanisms built during an 8-week MBCT program hold steady long after the treatment ends.
MBCT for Depression & Anxiety: Key Research Numbers at a Glance
Surprising Benefits of Mindfulness for Anxiety and Depression! Better than Medication?!
sbb-itb-23f89d4
Quick comparison
| Question | What the pooled research shows |
|---|---|
| Does MBCT help depression symptoms? | Yes, modestly |
| Does MBCT help anxiety symptoms? | Yes, modestly |
| Is it best for acute symptom treatment? | It can help, but effects are smaller against active care |
| Is it best for relapse prevention? | Yes – this is where support is strongest |
| Does it beat CBT or medication by a lot? | Usually no |
| Do benefits last? | Often yes, at least in available follow-up periods |
| Any limits in the data? | Yes – very high study-to-study variation and uneven study quality |
So when I read the meta-analyses, the main takeaway is simple: MBCT is not a cure-all, but it is a solid option for relapse prevention and a reasonable add-on for symptom relief.
What the Meta-Analyses Show for Current Anxiety and Depression Symptoms
Recent psychiatric reviews show that MBCT successfully reduces both depression and anxiety scores. The clearest clinical gains show up when MBCT is compared directly with waitlist controls or standard treatment-as-usual (TAU).
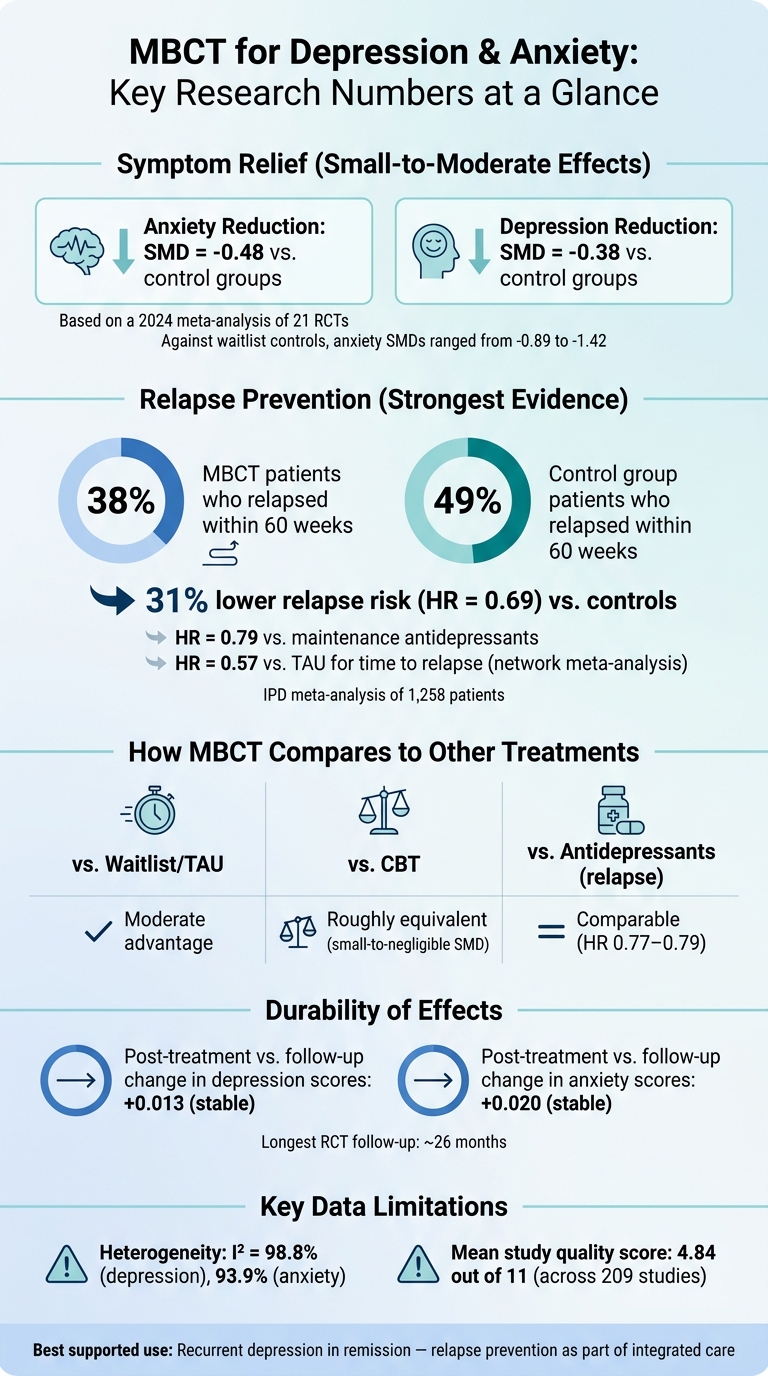
A comprehensive 2024 meta-analysis of 21 Randomized Controlled Trials (RCTs) reported a Standardized Mean Difference (SMD) of -0.48 for anxiety and -0.38 for depression versus control groups. Because anxiety and depression frequently co-occur, many of these clinical trials utilized mixed symptom samples, proving that mindfulness-based interventions actively target shared underlying neurobiological pathways.
The Comparator Catch: MBCT vs. Active Treatments
Taken together, these pooled results point to MBCT as a reliable, durable option for symptom relief. However, there is an important clinical catch: when MBCT is matched head-to-head against active mental health treatments—like traditional Cognitive Behavioral Therapy (CBT) or maintenance psychiatric medication—its statistical edge gets smaller.
Rather than wiping out symptoms completely on its own, MBCT acts as a powerful stabilizing force. That is why the strongest, most consistent clinical signal for MBCT shows up somewhere else: preventing future relapse.
The Strongest Signal: Relapse Prevention in Recurrent Depression
MBCT has its best, most robust clinical evidence in relapse prevention for individuals dealing with recurrent Major Depressive Disorder (MDD).
In a massive individual patient data (IPD) meta-analysis of 1,258 patients, only 38% of individuals who received MBCT relapsed within 60 weeks, compared with 49% of control groups. This represents a 31% lower risk of depressive relapse (Hazard Ratio of 0.69), according to a landmark IPD meta-analysis published in JAMA Psychiatry (Kuyken et al., 2016)
Even when evaluated against active medical treatments—including maintenance antidepressant medication—MBCT still successfully lowered the risk of relapse (HR 0.79). Furthermore, a network meta-analysis found a substantial advantage over treatment-as-usual for time to relapse (HR = 0.57) and over a placebo (HR = 0.23).
“Mindfulness-based cognitive therapy appears efficacious as a treatment for relapse prevention for those with recurrent depression, particularly those with more pronounced residual symptoms.” — Willem Kuyken, PhD
In medical practice, this means that while the statistical gap between MBCT and medication might look small on paper, the real-world impact over many months is profound for patients trying to stay well without increasing dosages.
Who Benefits Most From Mindfulness-Based Cognitive Therapy?
Looking past the broad statistical averages, the next step is determining which patient populations benefit most from an integrative mindfulness approach.
-
Recurrent MDD in Remission: The strongest clinical support for MBCT remains in adults with recurrent major depression who are currently in full or partial remission. The data shows that MBCT works regardless of how many prior depressive episodes a person has experienced.
-
High Residual Symptoms: Individuals who still carry lingering, low-grade depressive symptoms after recovering from an acute episode see the most significant preventative gains from MBCT.
-
Co-Occurring Anxiety: The research base is expanding rapidly beyond core depression. High-quality studies now include individuals dealing with mixed anxiety-depressive samples, social anxiety disorder, and Generalized Anxiety Disorder (GAD).
The Limitations of MBCT Data: A Grounded View
At Modyfi Health, we prioritize clinical candor over health trends. While MBCT is a highly effective clinical tool, the pooled scientific findings do come with clear limitations:
- Study-to-Study Variation: Large-scale meta-analyses frequently report high heterogeneity (I² values often exceeding 90% for depression and anxiety outcomes). This high level of statistical variation means that trial environments, patient groups, and therapist training varied widely across countries, so global averages must always be interpreted carefully.
- Clinical Screening is Essential: The vast majority of randomized controlled trials (RCTs) for MBCT intentionally leave out individuals with active bipolar disorder, psychosis, or severe neurocognitive disorders. Because these populations were excluded from the baseline data, MBCT should not be assumed as a safe standalone tool for them without specialized psychiatric oversight.
- Trauma Considerations: Standard 8-week MBCT group formats involve intensive focus on internal bodily sensations and thoughts. This approach requires close psychological monitoring—and often practical adaptations—for individuals experiencing acute trauma symptoms, PTSD, or active suicidality, as intense mindfulness can sometimes trigger hyperarousal.
(Source: Nandarathana & Ranjan, 2024. Systematic Review and Meta-analysis on MBCT Efficacy, Journal of Clinical Medicine / PMC11572415)”
How MBCT Fits Into Your Personalized, Whole-Person Care Plan
Given these scientific guardrails, MBCT makes the most practical sense inside a broader, comprehensive mental health framework. It delivers the best patient outcomes when utilized as part of an integrated psychiatric care plan, rather than a stand-alone cure.
In a functional psychiatric model, MBCT seamlessly pairs with:
-
Expert medication management tailored to your biology.
-
One-on-one traditional psychotherapy.
-
Gradual, clinically supervised antidepressant tapering protocols.
Mental health recovery is rarely accomplished through one single tool. MBCT provides the psychological framework to help you notice painful, anxious thoughts without getting pulled under by them, while our medical team treats the root causes of your symptoms.
FAQs
Who is MBCT best for?
MBCT is primarily engineered for individuals with recurrent Major Depressive Disorder who want to prevent future depressive episodes. However, modern research shows it is also a highly effective add-on for individuals managing chronic physical health conditions paired with co-occurring anxiety symptoms.
Can MBCT replace my psychiatric medication?
No, MBCT should not be viewed as a automatic substitute for prescription medication or standard therapy. Instead, it serves as an evidence-based, non-drug integrative tool. Decisions regarding your medication or tapering plans should always be made collaboratively with a qualified provider.
How long do the benefits of MBCT last?
Clinical follow-up data demonstrates that the emotional regulation skills gained during MBCT remain highly stable. In randomized controlled trials, symptom gains and lower relapse risks held firm throughout follow-up periods spanning up to 26 months.
Ready to Experience True Whole-Person Mental Health Care?
If you are ready to move beyond basic symptom management and build a resilient foundation for long-term health, Modyfi is here to support you. We protect your autonomy and make starting care as frictionless as possible:
-
Find Your Clinician: Explore our providers to book an integrated psychiatric appointment online today.
-
Not sure where to start? Book a FREE 15-minute Discovery Call with our care coordination team to map out your personalized path forward.
{kind=link}