
{kind=link}
Post-Traumatic Stress Disorder (PTSD) affects millions of individuals worldwide, necessitating diverse and adaptive clinical interventions. While traditional modalities such as prolonged exposure therapy and medication management remain clinical gold standards, emerging mental health technologies offer promising alternatives. Virtual Reality Exposure Therapy (VRET) represents a significant technological shift, providing immersive environments that allow patients to process trauma within a controlled, safe clinical setting.
Consequently, selecting the most appropriate therapeutic pathway requires a nuanced understanding of how these modern interventions compare to established methods. Evaluating efficacy, patient retention, and treatment duration is essential for achieving optimal, long-term recovery.
Furthermore, integrating advanced technological tools with comprehensive psychiatric care enhances the personalization of treatment plans. The following matrix provides a preliminary baseline comparison between Virtual Reality Therapy and traditional PTSD protocols:
Quick Comparison
| Metric / Feature | Virtual Reality Therapy (VRET) | Traditional Exposure Therapy | Medication Management |
| Primary Mechanism | Immersive digital immersion and controlled habituation. | Imagination-based recall and real-world exposure. | Biochemical symptom stabilization. |
| Patient Engagement | High visual and sensory engagement. | Dependent on patient’s imaginative capacity. | Passive adherence to daily dosing protocols. |
| Typical Duration | Often compressed (e.g., 6 to 12 sessions). | Standard (e.g., 8 to 16 weekly sessions). | Ongoing, long-term maintenance. |
| Clinical Control | Real-time environment manipulation by the clinician. | Dependent on verbal guidance and self-reporting. | Dependent on metabolic response and follow-ups. |
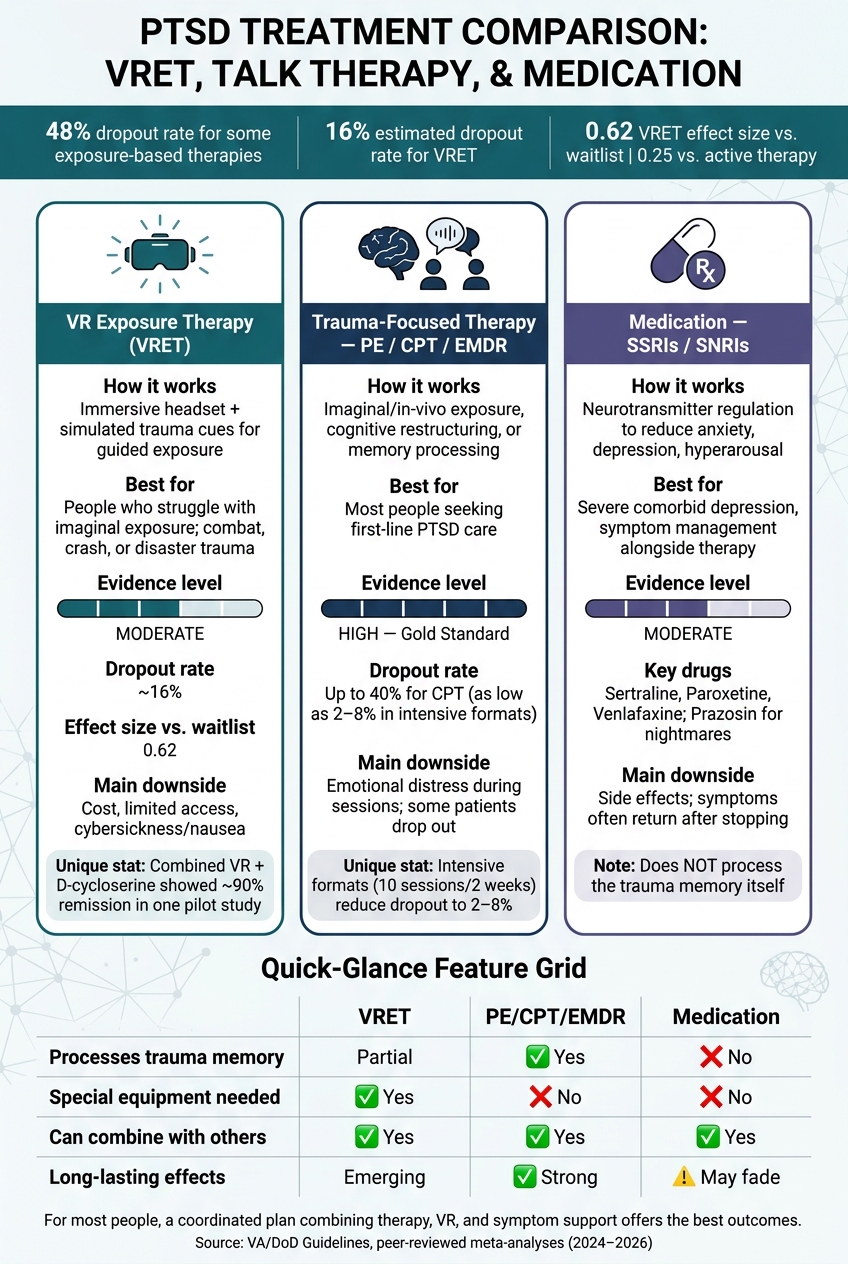
For many people, the most useful path is not one treatment by itself. It’s a care plan that combines therapy, symptom support, and close follow-up.
VR Therapy vs. Traditional PTSD Treatments: Key Stats & Comparison
Treating PTSD With Virtual Reality Therapy: A Way to Heal Trauma
sbb-itb-23f89d4
How Standard PTSD Treatments Work
In the U.S., PTSD care is built around trauma-focused psychotherapy. VA/DoD guidelines recommend it first because it improves core symptoms more than medication and its effects tend to last longer. That makes these therapies the main benchmark when people compare newer options like VR therapy.
Trauma-Focused Talk Therapies
The three most recommended therapies are:
- Prolonged Exposure (PE),
- Cognitive Processing Therapy (CPT),
- Eye Movement Desensitization and Reprocessing (EMDR)
They take different paths, but they aim at the same problem: helping patients work through trauma instead of steering clear of it.
PE slowly brings patients into contact with avoided memories and everyday triggers. CPT focuses on beliefs tied to safety, guilt, trust, and control. EMDR uses guided eye movements or tapping to help patients process traumatic memories without having to fully retell them out loud.
Medication Management for PTSD Symptoms
SSRIs such as sertraline (Zoloft) and paroxetine (Paxil), along with the SNRI venlafaxine (Effexor), are the main medication options for reducing PTSD symptoms. These drugs are used to treat symptoms like anxiety, depression, and hyperarousal. For trauma-related nightmares, prazosin is sometimes added as an adjunctive treatment.
A vital clinical consideration in psychiatric management is that the therapeutic gains achieved through medication alone often diminish once the pharmacological treatment is discontinued. For this reason, medication is rarely viewed as a standalone cure for PTSD.
Instead, pharmacotherapy is most effectively utilized as a stabilizing therapeutic bridge. By dampening acute symptoms like severe depression, cognitive fog, or debilitating insomnia, medication helps quiet the nervous system. This crucial stabilization places patients in a significantly better psychological and physiological position to actively engage in, tolerate, and benefit from intensive trauma-focused interventions like VR exposure therapy.
| Medication Type | Common Examples | Primary Clinical Target in PTSD |
| SSRIs | Sertraline (Zoloft), Paroxetine (Paxil) | Generalized anxiety, depressive mood, hyperarousal |
| SNRIs | Venlafaxine (Effexor) | Emotional regulation, panic, and intrusive thoughts |
| Alpha-1 Blockers | Prazosin | Trauma-related nightmares and sleep disturbances |
Key Benefits and Common Barriers
There’s a lot of research behind these treatments, but getting care in day-to-day practice can still be hard.
| Barrier Type | Examples |
|---|---|
| Therapy-related | Strong distress during sessions; limited access to trained clinicians |
| Medication-related | Side effects; symptoms returning after discontinuation |
| Systemic | Stigma, scheduling, and access delays |
Treatment Adherence and Retention Challenges
Patient dropout remains one of the most significant hurdles in trauma recovery. In standard clinical trials, traditional cognitive-behavioral approaches can see substantial attrition; for instance, some comparative studies have noted dropout rates around 40% for Cognitive Processing Therapy (CPT), whereas streamlined alternatives like Written Exposure Therapy (WET) often demonstrate significantly lower attrition, sometimes around 6%. Interestingly, formatting also plays a critical role in retention: intensive protocols—such as delivering 10 sessions over a condensed two-week span—have been shown to drastically reduce dropout rates to between 2% and 8%.
This clear disparity between clinical efficacy in controlled trials and real-world patient adherence underscores a critical gap in trauma care. It is precisely within this gap that Virtual Reality Exposure Therapy (VRET) commands attention, offering an immersive framework designed to maximize patient engagement and completion rates.
How VR Therapy for PTSD Works
Virtual Reality Exposure Therapy (VRET) uses the same core approach as traditional exposure treatments, but it does so through controlled digital simulations.
In practice, instead of asking a patient to rely solely on their imagination to recall a traumatic event—which can often feel abstract or overwhelming—the technology creates an interactive, visual, and auditory setting. For many individuals, visualizing these memories internally is incredibly difficult or leads to cognitive avoidance. Virtual reality bridges this gap by making trauma cues more concrete, making it easier and safer for patients to face and process their memories.
What Happens During a VR Exposure Therapy Session
Sessions typically last between 60 and 90 minutes. The process moves step-by-step, closely respecting the patient’s pace and comfort levels to ensure they feel safe from start to finish.
1.Preparation and Grounding:
What Current Research Says About VR Therapy’s Effectiveness
The scientific data surrounding Virtual Reality Exposure Therapy is highly encouraging, though researchers emphasize that the evidence base is still growing.
Clinical studies offer a clear look at how VRET performs in real-world psychiatric care:
-
Symptom Reduction: A comprehensive meta-analysis of 13 randomized controlled trials found a significant, moderate-to-large reduction in PTSD symptoms among patients using VR.
-
Targeted Military Success: Smaller studies focusing on Virtual Reality-Based Graded Exposure Therapy (VR-GET) have shown even more pronounced positive effects, particularly for combat-related trauma.
-
Equivalency to Standard Care: A 2026 Veterans Affairs (VA) review indicated that VR-assisted prolonged exposure performs comparably to traditional prolonged exposure for specific military groups, though researchers are still gathering long-term follow-up data.
The Takeaway: While standard exposure therapy currently holds a larger historical database of research, virtual reality is rapidly establishing itself as an equally effective, highly engaging alternative that helps bridge the gap for patients who struggle with traditional methods.
Benefits and Practical Limits of VR Treatment
Understanding both the clinical advantages and the practical boundaries of Virtual Reality Exposure Therapy helps patients make informed decisions about their care.
The Clear Advantages of VRET
-
Reduced Reliance on Imagination: Standard imaginal exposure requires patients to mentally reconstruct their trauma. In contrast, VR provides direct sensory input—including immersive visuals, synchronized sounds, and sometimes even physical vibrations or scents—making the therapeutic work feel more grounded and manageable.
-
Favorable Retention Rates: Clinical data estimates the patient attrition rate for VRET at approximately 16%, which competes closely with traditional trauma therapies.
-
Clear Dose-Response Pattern: Research consistently indicates a strong dose-response relationship, meaning that completing the full recommended sequence of sessions directly correlates with greater, more lasting treatment effects.
The Current Limitations
-
Technological Barriers: High equipment costs and technical requirements mean that many standard clinics cannot yet support VR setups.
-
Physical Discomfort: A small percentage of patients experience “cybersickness”—mild nausea, dizziness, or eye strain caused by the headset—which can temporarily disrupt a session.
-
Limited Access: Because VRET requires specialized clinical training, the number of qualified practitioners across the U.S. remains limited, leaving this advanced care out of reach for many communities.
Summary: While structural costs and specialized training limit widespread access, VRET’s ability to ground patients through sensory immersion makes it a highly effective tool for those who find traditional therapy difficult to navigate.
VR Therapy vs. Standard PTSD Treatments: Side-by-Side Comparison
This comparison matters because VR’s biggest edge is engagement, while standard care still has the strongest evidence base and the broadest access. The big split isn’t only how these treatments work. It’s also about fit: the patient’s symptoms, access to care, and comfort with exposure all shape what makes sense.
The table below lays out the main tradeoffs.
| Feature | VR Exposure Therapy (VRET) | Trauma-Focused Therapy (PE/CPT) | Medication (SSRIs/SNRIs) |
|---|---|---|---|
| Delivery Method | VR headset and immersive digital scenes | Imagined exposure or cognitive restructuring | Daily oral medication |
| Core Mechanism | Sensory-rich exposure to digital trauma cues | Imaginal/in-vivo exposure or cognitive restructuring | Neurotransmitter regulation |
| Evidence | Emerging/Moderate | High (gold standard) | Moderate |
| Likely Benefits | More engaging for people who struggle with imagery | Broadly effective; no special equipment needed | Easier to access; reduces anxiety, depression, and arousal symptoms |
| Limitations | Equipment costs; cybersickness; limited trauma scenarios | Requires emotional engagement and imagination | Side effects; symptoms may return if medication is stopped |
| Adherence | Lower in published studies | Higher across most formats | Varies |
| Ideal Use Case | Combat trauma, car crashes, natural disasters, or imaginal blocks | Complex trauma, high verbal ability, or limited tech access | Severe comorbid depression or symptom management while engaging in therapy |
How These Treatment Methods Differ in Practice
These treatments aim at the same problem, but they go after it in different ways. VR uses controlled sensory cues – visuals and sound inside a digital scene – to activate the fear memory. PE depends on imagined exposure to that same memory. CPT takes a different route: it focuses less on replaying the memory and more on the distorted beliefs tied to it. Medication works on symptoms such as anxiety, depression, and hyperarousal, rather than processing the trauma memory itself.
You can think of it this way: VRET tries to make the memory feel more present, PE asks the patient to bring it up in the mind, and CPT works on the meaning the patient has attached to it. SSRIs and SNRIs, meanwhile, can lower the day-to-day symptom load.
Effectiveness, Safety, and Dropout Rates
The evidence gap between VR and standard talk therapy is real, but it is smaller than many people assume. A comprehensive meta-analysis found that VRET produced a significant effect size of $0.62$ compared with waitlist controls, but a non-significant effect size of $0.25$ when compared head-to-head with active standard therapies. Consequently, while VR consistently outperforms non-active controls, it has not yet shown a steady pattern of outperforming PE or CPT directly.
Understanding Retaining and Safety
Patient retention is another important piece of the clinical picture:
-
Attrition Rates: Published studies indicate somewhat higher dropout rates for VR therapy compared to standard trauma-focused therapies. This is an important consideration, as a treatment cannot deliver its full benefits if a patient stops the protocol early.
-
A Reassuring Safety Profile: Regarding patient safety, the data is highly reassuring. No major meta-analyses have tied VR therapy to serious adverse effects, such as increased suicide risk or lasting symptom worsening.
VRET stands as a safe and statistically effective option for trauma recovery. While it performs comparably to traditional methods rather than outperforming them, it remains a powerful alternative—provided patients complete their full course of care.
Who May Do Better With Each Approach
Fit matters as much as the treatment label. VRET tends to help people who hit a wall during imaginal exposure – people who can’t form a clear picture of the trauma, or who feel detached from it in standard talk therapy. It also makes more sense for trauma types that are easier to simulate, such as combat, car crashes, or natural disasters.
Standard therapies are often the better choice when the trauma is harder to simulate, when VR-equipped care isn’t easy to access, or when comorbidities make a broader talk-therapy approach more practical. Medication usually fits best as symptom management and as an adjunct to therapy.
Can VR and Standard Treatments Work Together?
PTSD care often yields the best results when structured in clinical stages, allowing virtual reality and traditional treatments to work side by side. In many clinical settings, this integrative approach represents the most practical and comprehensive path to recovery.
Rather than competing with one another, each modality addresses a distinct layer of the healing process:
-
VRET provides the structured, immersive environment needed to safely confront and desensitize core trauma memories.
-
Standard Talk Therapy (like CPT) helps the patient process the broader cognitive meaning of the event and rebuild daily coping mechanisms.
-
Medical Management stabilizes the nervous system by reducing acute biochemical symptoms like hyperarousal and panic.
By combining these strengths, an integrative care plan ensures that a patient is not just processing their past trauma, but is also equipped with the cognitive and physiological support needed to sustain long-term wellness.
Why a Combined Care Plan May Be the Most Practical Option
VR and talk therapy can support each other well. A combined session may run about 90 minutes, with 30 to 45 minutes of VR exposure followed by 30 minutes of processing. The VR portion brings up the fear memory through targeted sensory cues, while the talk therapy component helps the patient sort through what emerged and put the experience into words.
Medication can also play a supportive role. SSRIs may help steady biochemical symptoms during treatment. Additionally, clinical studies have evaluated D-cycloserine (DCS)—taken 30 to 90 minutes before VR—to facilitate extinction learning (the cognitive process of unlearning a fear response).
The World Trade Center Study: In a notable pilot study conducted by Weill Cornell Medicine evaluating World Trade Center survivors, pairing VR therapy with DCS was linked to a remission rate of approximately 90%. While the study relied on a small sample size and requires further large-scale validation, the clinical signal remains highly significant.
However, not every medication aligns well with exposure-based therapy. Benzodiazepines like alprazolam may actually weaken the therapeutic effects of VR exposure by suppressing the physiological response necessary for emotional processing.
Finally, day-to-day habits matter just as much. Consistent sleep, regular exercise, and proper nutrition heavily shape both active treatment engagement and long-term recovery.
Key Takeaways
Standard trauma-focused therapies like Prolonged Exposure and CPT are still the most established PTSD treatments. VR therapy looks promising, especially for patients who struggle with imaginal exposure or who also have depression, but it tends to work best as one part of a bigger plan, not as a stand-alone answer. The right path depends on symptoms, support systems, and treatment goals. For many people, the most workable option is a coordinated plan that uses both.
How Modyfi Health Can Support Ongoing PTSD Recovery
Integrative Trauma Care at Modyfi Health
Technology like Virtual Reality Exposure Therapy (VRET) is a powerful tool for confronting trauma, but true healing requires more than an isolated intervention. At Modyfi Health, we understand that PTSD reshapes both the mind and the body. That is why we don’t just offer therapy; we provide a fully integrated, whole-person care model designed to support you at every stage of your recovery.
Our collaborative approach brings together multiple clinical disciplines under one roof to build a foundation for sustainable growth:
-
Targeted Psychiatry & Medication Management: We monitor and stabilize the biochemical symptoms of trauma—such as hyperarousal, insomnia, and panic—ensuring your nervous system is resilient enough to engage deeply in exposure work.
-
Advanced Lab Work & Functional Assessment: Trauma impacts your physiology. We look beneath the surface, evaluating metabolic markers, hormonal health, and nutritional deficiencies that could be stalling your energy and recovery.
-
Evidence-Based Psychotherapy: Whether utilizing cutting-edge immersive tech like VRET or foundational cognitive processing, our specialized therapists guide you safely through your memories and help you rebuild meaningful daily coping strategies.
-
Lifestyle & Functional Support: Long-term wellness is sustained outside the clinic. We integrate personalized guidance on sleep architecture, physical movement, and metabolic nutrition to ensure your body has the baseline fuel to heal.
Ready to Take the Next Step?
Recovery from PTSD is not a one-size-fits-all process, and you don’t have to navigate it alone. Our team is ready to map out a comprehensive, multidisciplinary care plan tailored to your unique clinical profile and goals. Schedule a Consultation with a Modyfi Health Specialist Today.
FAQs
Is VR therapy a first-line PTSD treatment?
No. VR therapy is not currently classified as a first-line treatment for PTSD; traditional trauma-focused therapies like Prolonged Exposure (PE) and Cognitive Processing Therapy (CPT) hold that status.
Clinical research suggests that VRET serves as a viable, evidence-based alternative to standard imaginal exposure rather than a superior replacement. Head-to-head studies generally show that VR-based exposure yields comparable clinical outcomes to non-VR exposure therapy, with some data suggesting a slight edge for traditional formats depending on the patient’s profile.
Who is most likely to benefit from VR therapy?
VR therapy may be especially beneficial for patients experiencing co-occurring PTSD and depression. It is also highly effective for individuals who struggle with traditional imaginal exposure—specifically those who find it difficult to mentally visualize their trauma or feel detached during standard therapy.
Because VR provides an immersive, controlled, and multisensory environment, it helps patients connect with their emotions more safely and consistently, offering a repeatable way to process traumatic memories under close clinical supervision.
Can PTSD medication and VR therapy be used together?
Yes. Medication and virtual reality therapy can absolutely be utilized together. Clinical frameworks frequently pair pharmacological support with exposure-based protocols to optimize patient outcomes.
Because PTSD presents unique challenges for every individual, clinicians typically tailor treatment plans using a combination of evidence-based modalities. At Modyfi Health, our integrative care model is designed to support comprehensive, whole-person treatment plans that seamlessly blend psychological, technological, and medical interventions.
Can VR therapy cause motion sickness or “cyber sickness”?
Yes, some patients may experience temporary “cyber sickness,” which includes symptoms like mild nausea, dizziness, or eye strain. However, in a clinical setting, this risk is minimal. Specialized therapeutic VR software uses high refresh rates and fixed visual reference points designed to reduce sensory conflict. Additionally, clinicians are trained to monitor patients closely, pace the exposure intervals, and use grounding techniques to ensure the session remains comfortable and safe.
How many sessions of VR therapy are usually needed for PTSD?
While treatment plans are fully customized to the individual, a standard VRET protocol typically ranges from 8 to 12 weekly sessions, each lasting between 60 and 90 minutes. Because VRET is a structured, short-term intervention, patients often begin noticing a reduction in hyperarousal and avoidance behaviors within the first few weeks, provided they consistently engage in the processing phases that follow the VR exposure.
What is the difference between Virtual Reality Therapy and standard Imaginal Exposure?
Traditional Imaginal Exposure requires the patient to close their eyes and mentally reconstruct their traumatic memory using their imagination, guided by a therapist’s voice. Virtual Reality Exposure Therapy (VRET) replaces the need for mental visualization by using an immersive headset to generate precise computer-generated environments (such as specific combat zones or generic trauma contexts). This makes the therapy highly accessible for individuals who tend to emotionally block out or struggle to recall visual details of their trauma.