
{kind=link}
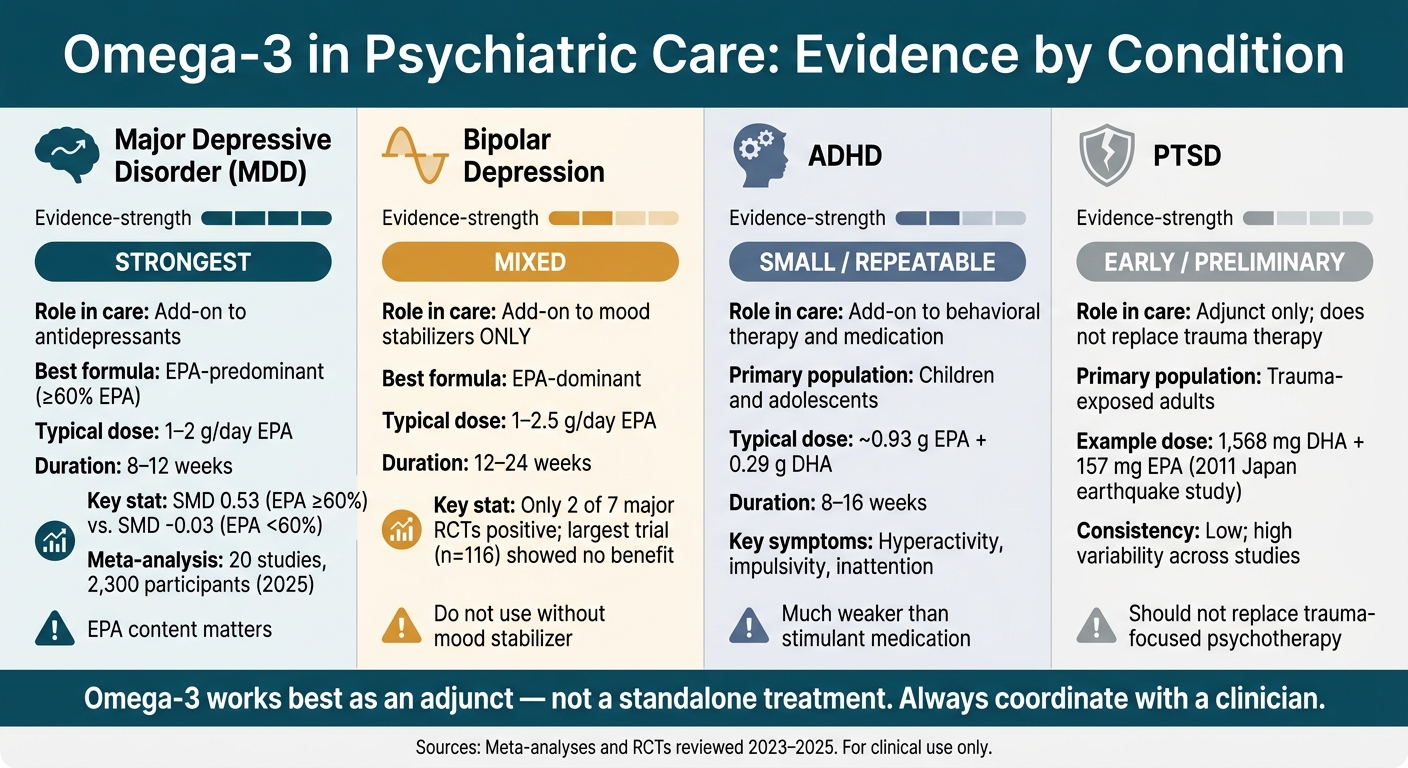
When examining the role of omega-3 fatty acids in psychiatric care, clinical evidence indicates that its utility varies significantly by condition. The strongest therapeutic signal appears in the treatment of unipolar depression, whereas the data remains less definitive for bipolar depression, demonstrates modest effects in ADHD, and is still in the preliminary stages for PTSD.
To summarize the current state of clinical research, the evidence maps out as follows:
-
Major Depressive Disorder (MDD): Demonstrates the highest level of clinical support, particularly when utilizing EPA-predominant formulations.
-
Bipolar Depression: Yields mixed outcomes and is clinically indicated only as an adjunctive support alongside an established mood stabilizer.
-
ADHD: Shows modest symptom improvements, observed primarily within child and adolescent populations.
-
PTSD: Characterized by early data and highly mixed findings; it does not serve as a primary intervention.
Critical Formulation and Dosing Variables
Several critical nuances in formulation significantly dictate clinical success. In major depression studies, omega-3 products containing at least 60% EPA demonstrated substantially higher efficacy than low-EPA alternatives. A comprehensive 2025 meta-analysis encompassing 20 distinct studies and 2,300 participants confirmed a pooled improvement in depressive symptoms, though clinical outcomes varied sharply based on the specific formula used. In clinical practice, the standard adjunctive dosing strategy for MDD typically ranges between 1 to 2 grams per day for a duration of 8 to 12 weeks.
The fundamental takeaway for integrative care is clear: omega-3 fatty acids are most effectively utilized as an adjunct alongside psychiatric medication, psychotherapy, or both—rather than as a standalone treatment. While associated side effects are generally mild, screening for individual bleeding risks and verifying product quality remain essential steps prior to implementation.
Omega-3 in Psychiatric Care: Evidence Strength by Condition
Omega-3 Fatty Acids for Mood Disorders and Other Psychiatric Conditions
sbb-itb-23f89d4
Quick Comparison
| Condition | What the research suggests | Best fit in care | Main caution |
|---|---|---|---|
| MDD | Strongest support | Add-on to antidepressants | EPA content matters |
| Bipolar depression | Mixed | Add-on to mood stabilizers | Do not use on its own |
| ADHD | Small, repeatable effects | Added support with standard care | Much weaker than stimulants |
| PTSD | Early and mixed | Add-on only | Should not replace trauma therapy |
This initial matrix establishes the core baseline for how omega-3 fatty acids integrate into modern psychiatric protocols. The remainder of this clinical review provides an explicit, evidence-based breakdown of targeted patient populations, specific therapeutic dosages studied in clinical trials, and the clear operational boundaries of nutritional psychiatry
Evidence in Mood Disorders: Unipolar Major Depression vs. Bipolar Depression
Major Depressive Disorder: Strongest Case for EPA-Dominant Add-On Use
Major Depressive Disorder (MDD) presents the clearest therapeutic signal in psychiatric literature. Consistent with international clinical consensus data, an analysis of 20 randomized controlled trials encompassing over 2,300 participants demonstrates a pooled clinical benefit for depressive symptoms, although outcomes shift dramatically based on the specific molecular formulation utilized. Reported effect sizes vary between 0.10 and 0.61, highlighting how profoundly study design and EPA concentrations dictate patient outcomes.
The clinical pattern is definitive: EPA-predominant formulations yield significantly superior outcomes, particularly when the product maintains a concentration of at least 60% EPA. Statistical analyses reveal a stark contrast in clinical efficacy:
-
Formulations meeting or exceeding the 60% EPA threshold demonstrated a Standardized Mean Difference (SMD) of 0.53.
-
Formulations falling below the 60% EPA threshold generated an SMD of -0.03, representing an absolute absence of therapeutic benefit.
Formulations containing exclusively DHA, or those maintaining low EPA ratios, have failed to demonstrate steady clinical utility. Consequently, literature supports the application of omega-3 fatty acids strictly as an adjunctive intervention rather than a monotherapy. The standard psychiatric dosing protocol involves 1 to 2 grams per day of pure EPA for a duration of 8 to 12 weeks, paired directly with prescribed antidepressant medication.
It is necessary to note a clinical caveat: early psychiatric trials likely inflated initial effect sizes due to publication bias and high statistical heterogeneity. By comparison, the therapeutic signal for treating bipolar depression remains considerably weaker and less consistent.
Bipolar Depression: Mixed Results and Mandatory Coordination with Mood Stabilizers
The clinical dataset evaluating bipolar depression is noticeably smaller, and the corresponding therapeutic outcomes remain highly mixed. While a meta-analysis of six randomized controlled trials (RCTs) indicated a modest improvement in depressive symptoms with no adverse effect on mania, a deeper review reveals a complex clinical landscape.
Omega-3 supplementation for this population must be utilized exclusively as an adjunct to established mood stabilizers. The evidence base remains fragile; only 2 out of 7 major clinical RCTs yielded positive outcomes, and the largest structured trial ($n = 116$) demonstrated zero clinical benefit over a placebo. Typical therapeutic interventions evaluated in literature range from 1 to 2.5 grams per day of EPA over an extended course of 12 to 24 weeks.
From a safety perspective, clinical data has not identified a clear treatment-emergent “mania-switch” signal, which is a vital consideration in bipolar care. However, because sample sizes across these specific trials remain structurally small, the comprehensive safety and tolerability profile is not entirely settled.
“Evidence of efficacy of omega-3 supplementation in treating bipolar mania is minimal.” – Madeeha Nasir, Therapeutic Advances in Psychopharmacology
Side-by-Side Comparison: Major Depressive Disorder vs. Bipolar Depression
The clinical operational differences between these two mood disorders become evident when evaluating their specific formulation requirements, therapeutic dosages, and overall role within a psychiatric treatment plan.
| Feature | Major Depressive Disorder | Bipolar Depression |
|---|---|---|
| Evidence strength | Strongest evidence for EPA-dominant adjunctive use | Mixed; smaller evidence base |
| Primary formulation | EPA-predominant, at least 60% EPA | EPA-dominant |
| Typical EPA dose | 1–2 g/day | 1–2.5 g/day |
| Typical duration | 8–12 weeks or longer | 12–24 weeks in many trials |
| Role in care | Adjunct to antidepressants | Adjunct to mood stabilizers |
| Symptom focus | Depressive symptoms | Depressive symptoms; no clear effect on mania |
| Safety concerns | Mostly mild gastrointestinal side effects | Generally well tolerated; no clear mania-switch signal |
The therapeutic outcomes observed in these primary mood disorders remain substantially robust when compared to the more preliminary data available for neurodevelopmental and trauma-related conditions
Evidence in ADHD and PTSD
Compared with depression, the evidence for ADHD and PTSD is smaller and more mixed.
ADHD: Small but Repeatable Effects, Mainly in Children and Adolescents
Once you move beyond mood disorders, the signal gets weaker. Still, ADHD stands out with a small but repeatable effect. And just like in depression, omega-3 works as an add-on, not a main treatment.
Multiple meta-analyses show small, repeatable improvements in ADHD symptoms, especially in children and adolescents. The main areas affected are hyperactivity, impulsivity, and inattention. One trial using 0.93 g EPA and 0.29 g DHA improved impulsive dyscontrol. Most trials use EPA-rich or mixed EPA+DHA products for about 8 to 16 weeks.
That said, omega-3 is still weaker than stimulant medication. Its place is alongside behavioral therapy and medication, not instead of them.
PTSD: Early and Mixed Evidence, Not a Primary Treatment
PTSD is less consistent than ADHD, and the evidence is still at an early stage. The data come from only a small number of trials, and those studies use different EPA:DHA ratios, which makes the picture harder to read.
Conclusions remain tentative. For example, in survivors of the 2011 Japan earthquake, 1,568 mg DHA and 157 mg EPA helped women but not men. Researchers think omega-3 may help by reducing inflammatory signaling and supporting neuroplasticity, but the clinical evidence is still limited.
⚠️ Important: Omega-3 should not replace trauma-focused psychotherapy or other established treatments; it fits only as an adjunct.
Side-by-Side Comparison: ADHD vs. PTSD
| Feature | ADHD | PTSD |
|---|---|---|
| Evidence strength | Small but repeatable; supported by multiple meta-analyses | Preliminary and mixed; few clinical trials available |
| Primary population | Youth | Trauma-exposed adults and survivors |
| Consistency of findings | Higher consistency across studies | Lower; high variability in study design |
| Key symptoms targeted | Hyperactivity, impulsivity, inattention | Inflammatory signaling and fear-memory processing |
| Typical duration | 8–16 weeks | Varies; often focused on acute post-trauma windows |
| Proposed mechanism | Attention and impulse-control signaling | Inflammation and neuroplasticity |
| Role in care | Alongside behavioral therapy and medication | Adjunct to trauma-focused psychotherapy |
Cross-Condition Comparison, Dosing, and Safety
Where the Evidence Is Strongest Across Conditions
Across these conditions, the pattern is pretty straightforward: the case is strongest in depression, less clear in bipolar depression, modest in ADHD, and still early in PTSD. That order should shape how clinicians think about omega-3 as an add-on across diagnoses.
| Condition | Evidence Strength | Clinical Support Level |
|---|---|---|
| Major Depressive Disorder | Strongest / Consistent | Strong support for adjunctive use |
| Bipolar Depression | Mixed / Limited | Limited support for adjunctive use |
| ADHD | Small / Repeatable | Insufficient evidence for routine use |
| PTSD | Preliminary / Mixed | Minimal evidence |
Dosing Patterns, EPA:DHA Ratios, and Monitoring Steps
For mood disorders, the dosing range studied most often is 1–2 g/day of combined EPA+DHA, with EPA making up at least 60% of the blend. This high-EPA ratio is a crucial factor, as it is the specific feature most often linked with clinical benefits in depression trials.
For monitoring, the Omega-3 Index is the preferred biomarker because it measures EPA+DHA levels in red blood cells, which reflect long-term intake across their roughly 120-day lifespan. An index of 8–11% is considered optimal, while the Western population average usually falls between 2.9% and 7.7%.
A simple dietary review helps as well. If a patient already eats a lot of fish, that changes the starting point, since higher fish intake is naturally linked with lower rates of depression and anxiety.
Safety, Side Effects, and Medication Interactions
The main clinical caution is bleeding risk. Patients using anticoagulants, those with an underlying bleeding disorder, or anyone with an upcoming surgery should be thoroughly screened before higher doses are recommended.
Product quality also matters significantly. Some over-the-counter omega-3 products are oxidized, so it is highly recommended to use quality-tested formulations stabilized with an antioxidant such as vitamin E.
When omega-3 is added to antidepressants, studies demonstrate positive synergistic effects.
⚠️ Clinical Guidance: Despite these benefits, supplementation must always be coordinated with the treating clinician, especially when a patient has a more complex medical history.
These distinct factors help determine exactly when and how omega-3 safely fits into a broader psychiatric care plan.
Using Omega-3 in Integrative Psychiatric Care
When and How Clinicians May Add Omega-3 to a Care Plan
The clinical evidence is strongest for depression and weaker for ADHD and PTSD, so its practical use should always match the specific diagnosis and treatment setting. In most cases, omega-3 works best as an adjunct, not a standalone option. This is especially true in Major Depressive Disorder (MDD) when a patient still struggles with residual symptoms after starting antidepressants.
For children and adolescents with ADHD, clinicians may consider omega-3 as added support for symptoms like impulsivity or aggression alongside behavioral care or standard medication. The therapeutic dose must always match the diagnosis, current medications, and how the individual responds over time.
Because of these unique clinical variables, a coordinated care approach is essential for achieving the best outcomes.
How Modyfi Health Supports a Coordinated Approach
At Modyfi Health, board-certified psychiatrists, clinical nutritionists, and therapists work together to coordinate your evaluation, medication management, nutrition therapy, and functional diagnostic testing. When appropriate, specialized red blood cell membrane testing can be utilized to accurately identify low EPA and DHA levels.
This seamless coordination ensures that omega-3 supplementation remains a targeted, integrated part of your personalized care plan—rather than just another supplement you navigate on your own without professional guidance.
Ready to Build Your Personalized Care Plan?
Nutritional support works best when it is backed by science and coordinated by professionals. The multidisciplinary team at Modyfi Health is ready to help you seamlessly integrate evidence-based tools into your mental health journey.
➡️ Meet a Modyfi Provider Today and start your care plan
Key Takeaways
In practice, omega-3 should support standard psychiatric treatment, not replace it. Evidence is strongest for adjunctive use in MDD, more limited in bipolar depression, and still early in ADHD and PTSD. Bipolar depression calls for more caution because mood stabilizer coverage matters. Omega-3 should be used only alongside evidence-based psychiatric care, with screening for bleeding risk, drug interactions, and tolerance.
FAQs
How long does omega-3 take to help mood symptoms?
Clinical trials evaluating omega-3 as an add-on treatment for major depressive disorder typically study outcomes over a period of 8 to 12 weeks. While individual response timelines can vary based on the severity of the condition, consistency over this multi-week window is key to evaluating its effectiveness. Patients should always work with their clinical care team to safely track progress and adjust their treatment plan over time.
How do I choose an EPA-rich omega-3 supplement?
Look for a high-quality supplement from a trusted manufacturer that provides a total dose of 1 to 2 grams of pure EPA per day. Clinical consensus guidelines explicitly recommend using either a pure EPA product or an EPA/DHA blend where the formula contains at least 60% EPA (or an EPA-to-DHA ratio above 2:1). At Modyfi Health, clinicians help match specific nutritional support directly to your broader psychiatric care plan.
Who should avoid omega-3 or ask a doctor first?
While omega-3 supplements are usually low-risk and well-tolerated, you must consult a doctor first if you take anticoagulants (blood thinners), have an underlying bleeding disorder, or have an upcoming surgery, due to a potential increase in bleeding risk. Professional monitoring is also essential if you are navigating a severe mental health condition, ensuring nutritional support works safely alongside your standard medical care, never in place of it.
Can I take omega-3 instead of my prescribed antidepressant?
No. Clinical research is very clear that omega-3 fatty acids should be used strictly alongside medication, therapy, or both—not as a standalone treatment. It acts as a supportive catalyst to enhance the effects of standard psychiatric care, but it does not have the clinical strength to replace prescribed antidepressants or primary treatment protocols.
Does omega-3 help with anxiety or panic attacks?
While the strongest clinical evidence for omega-3 exists for major depression, population data shows that a higher dietary fish intake is generally linked with lower overall rates of both depression and anxiety. For acute anxiety or panic, omega-3 may support general neuroplasticity and reduce underlying inflammatory signaling, but it is typically integrated as a baseline lifestyle tool rather than a treatment for acute panic symptoms.
Why is over-the-counter omega-3 quality so important?
Many standard over-the-counter omega-3 supplements are prone to oxidation, which significantly reduces their effectiveness and can cause an unpleasant taste or stomach upset. It is highly recommended to select quality-tested, third-party-verified formulations that are stabilized with an antioxidant like vitamin E. Coordinated diagnostic testing, such as measuring your red blood cell membrane status, can help ensure your body is actually absorbing the right nutrients.