
When evaluating melatonin vs sleep hygiene for adhd, the most effective approach to managing sleep issues is to optimize daily habits first, and then consider supplementation if a delayed internal body clock continues to disrupt bedtime.
For many children with ADHD, sleep difficulties go far beyond a simple refusal to go to bed. It is usually a complex combination of late biological sleep timing, bedtime resistance, evening screen use, and the timing of stimulant medications.
Clinical research shows that melatonin can help children fall asleep about 16 minutes sooner on its own, but that baseline jumps to about 60 minutes sooner when it is paired with consistent sleep habits. However, it is vital to note that melatonin does not treat daytime ADHD symptoms, and long-term safety questions for pediatric use are still not fully answered.
The Quick Guide for Parents
1. Sleep Hygiene and Melatonin Do Different Jobs
-
Sleep hygiene focuses directly on daily habits, consistent schedules, and the physical bedroom environment.
-
Melatonin acts as a biological timing tool that signals the body clock that it is time to rest.
2. Sleep Hygiene Protocols Should Come First
-
Establish a fixed wake time every single day.
-
Introduce a screen-free wind-down routine for 30 to 60 minutes before bed.
-
Keep the bedroom dark and cool, ideally between 65°F and 68°F.
-
Ensure there is no caffeine consumption after 3:00 p.m.
-
Prioritize morning bright light exposure and physical exercise earlier in the day.
3. Melatonin Can Help When Routines Are Not Enough
-
It serves as the best fit for children experiencing a true delayed sleep phase.
-
Associated side effects are typically mild, such as temporary morning grogginess or minor headaches.
-
Product quality and exact dosages can vary significantly in the U.S. because it is regulated as a dietary supplement.
4. The Best Results Come From Combining Both Strategies
-
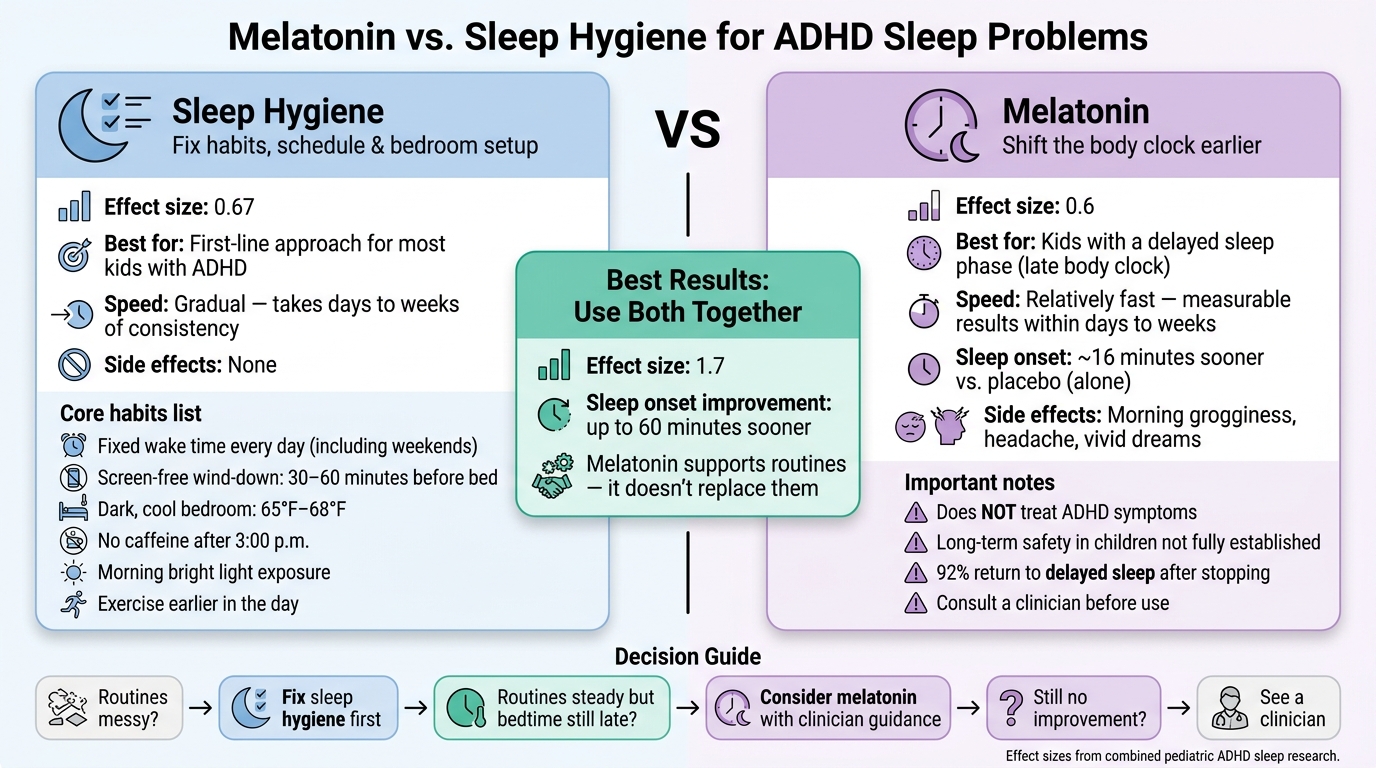
Sleep hygiene alone demonstrates a meaningful clinical effect size of 0.67.
-
Melatonin alone demonstrates an effect size of 0.6.
-
Combined treatment yields a much more powerful effect size of 1.7.
Regular use of melatonin as a sleep aid for kids raises concerns
Quick Comparison
| What to compare | Sleep Hygiene | Melatonin |
|---|---|---|
| Main job | Fixes habits and sleep setup | Shifts sleep timing earlier |
| Best use | First step for most kids with ADHD | When a late body clock is part of the problem |
| How fast it may help | Takes days to weeks of steady use | Often starts helping within days to weeks |
| Effect on falling asleep | Can help on its own | About 16 minutes sooner vs. placebo |
| Best result | Works best when done every day | Works best when added to routines |
| Downsides | Hard to keep up when families are tired | Mild side effects; long-term questions remain |
My takeaway: if routines are messy, fix those first. If routines are steady and sleep is still late, talk with a clinician before adding or increasing melatonin.
Melatonin for ADHD-Related Sleep Problems
Melatonin is a natural hormone made by the pineal gland that helps regulate the sleep-wake cycle. It acts more like a body-clock signal than a traditional sleeping pill. For children with ADHD, melatonin supplements may help move biological sleep timing earlier in the evening.
This intervention makes the most sense when sleep trouble is directly tied to a late body clock, rather than just weak bedtime habits. Therefore, melatonin is best seen as a strategic timing tool, not a standalone fix on its own.
What Melatonin Can and Cannot Do
Melatonin has a highly specific function. Research shows it can cut the time it takes a child to fall asleep by about 16 minutes on its own, and by as much as 60 minutes when it is paired with steady sleep habits. It may also make bedtime more predictable, which can significantly relieve stress for families stuck in the same nightly battle.
What melatonin cannot do is treat the core symptoms of ADHD. It does not improve daytime inattention, impulsivity, or hyperactivity. Melatonin helps exclusively with when a child falls asleep, but not with the underlying mechanisms of ADHD itself.
There is also a practical issue in the United States: melatonin is sold as a dietary supplement, meaning product strength, labeling, and purity can vary across brands. Interestingly, lower doses taken several hours before bed often work better than larger doses taken right at bedtime. Because both dose and timing matter immensely, it is highly recommended to seek guidance from a qualified clinician.
Safety, Side Effects, and Parent Concerns
For most children, short-term melatonin use is well-tolerated. Side effects are usually mild and may include morning grogginess, headaches, and vivid dreams. If a child appears groggy the following day, that often points to a dose that is either too high or taken too late in the evening.
The primary clinical concern involves long-term use. Currently, there is insufficient long-term data regarding how extended pediatric melatonin use might affect hormonal development or puberty. Furthermore, one long-term follow-up study discovered that 92% of children returned to their original delayed sleep patterns after stopping melatonin supplementation.
This high relapse rate highlights why professional clinician guidance is so important. A provider can help families determine whether melatonin is appropriate, establish the proper dosage, and decide how long to continue using it. This is also exactly why foundational bedtime routines and a supportive sleep environment remain irreplaceable.
sbb-itb-23f89d4
Sleep Hygiene for Children with ADHD
Sleep hygiene is much bigger than just a bedtime routine. It covers daily habits, physical environment, and lifestyle patterns that melatonin cannot fix on its own. Put simply, it deals with the conditions that make natural sleep possible in the first place. When these essential pieces are established, melatonin tends to work much more effectively if added later.
Practical Sleep Hygiene for ADHD:
-
Fixed Wake Times: The absolute starting point is a fixed wake time every day, including weekends, to help consistently reset the body clock. This single habit is incredibly powerful for long-term regulation.
-
Screen-Free Wind-Down: A screen-free wind-down for 30 to 60 minutes before bed is vital. Blue light from devices suppresses the body’s natural melatonin production, and screens add extra mental stimulation right when a child needs to slow down. This is a frequent hurdle, as one ADHD sleep study noted that 66.6% of children reported watching television as their main activity right before bed.
-
Optimized Bedroom Environment: The bedroom environment should support, not fight, sleep. Keeping the room dark and cool helps facilitate the body’s natural drop in temperature that signals it is time to rest.
-
Daytime Support: Incorporating bright morning light exposure, ensuring there is no caffeine intake after 3:00 p.m., and scheduling physical exercise earlier in the day all work in harmony to build natural sleep drive.
How Sleep Hygiene Helps Beyond Bedtime
When looking at the broader picture for adhd, the upside of focusing on habits goes far beyond simply falling asleep more easily. Establishing consistent and structured sleep routines can slightly reduce daytime ADHD symptoms, lessen behavioral challenges, lower overall family stress, and improve your child’s day-to-day functioning.
Why Families Often Struggle to Stick with It
This is where implementing behavior changes often becomes difficult. Bedtime pushback, caregiver fatigue, and a child’s late biological circadian rhythm can all make it incredibly tough to keep routines going consistently. On top of that, behavior adjustments usually take several weeks before they show a steady, measurable effect, which can feel deeply discouraging when exhausted families want relief immediately.
This delay in visible progress is exactly why foundational sleep hygiene must usually be prioritized before introducing or increasing melatonin, even when parents are naturally hoping for a faster solution.
Melatonin vs Sleep Hygiene for ADHD: Quick Comparison
Melatonin vs Sleep Hygiene for ADHD: Which Works Better?
Neither option does the entire job by itself. Sleep hygiene focuses directly on daily habits and the physical bedroom setup, while melatonin helps move the biological body clock earlier. For most families, the main challenge is figuring out what is actually driving the sleep issue: inconsistent routines or a delayed circadian rhythm.
You can use this comparison table to help match the right tool to your child’s specific sleep problem:
| Feature | Sleep Hygiene | Melatonin |
|---|---|---|
| Best fit | First-line for pediatric insomnia in ADHD | Ongoing trouble falling asleep, especially with a late body clock |
| How fast it works | Gradual; requires consistency over weeks | Relatively fast; measurable results within days to weeks |
| Effect on sleep onset | Moderate reduction in latency | Significant reduction; about 16 minutes vs. placebo |
| Side effects / risks | None | Usually mild; possible grogginess, headache, or vivid dreams |
When Sleep Hygiene Should Come First
If both daily habits and biological sleep timing are off, it is highly recommended to start with structured routines. A steady wake time, a predictable wind-down period, and a low-stimulation bedroom environment help the brain and body receive the exact same biological signal night after night. This foundational consistency matters far more than many parents expect.
In fact, clinical studies found that focusing on sleep hygiene alone produced an effect size of 0.67 in reducing initial insomnia. This represents a meaningful, measurable improvement in sleep quality before any type of supplement is ever added to the child’s routine.
When Melatonin May Be Worth Considering
If daily routines are already steady and bedtime still drifts late, incorporating melatonin may be the appropriate next step. This biological approach matters most when there are clear signs of a delayed circadian phase (a late internal body clock), which is a common challenge in children with ADHD.
It also makes practical sense to consult with a clinician if the timing of stimulant medications is suspected to be part of the sleep issue. In many cases, adjusting the daytime medication schedule with your prescriber is necessary before adding any type of over-the-counter sleep aid to your child’s routine.
What Combined Treatment Often Looks Like
The most powerful clinical results happen when melatonin is used to support structured sleep hygiene instead of replacing it. Research shows that a combined treatment protocol yields an impressive effect size of 1.7. This is a massive leap compared to an effect size of 0.67 for sleep hygiene alone, or 0.6 for melatonin alone.
Furthermore, combining these strategies resulted in a mean decrease in sleep-onset time of 60 minutes.
A highly effective and practical approach is straightforward: start by solidifying daily routines and bedroom habits first. If the time it takes your child to fall asleep is still lagging after those habits are steady, you can then talk to your clinician about adding a low dose of melatonin 30 to 60 minutes before bedtime.
Conclusion: Start with Routines, Add Melatonin Carefully When Needed
Sleep problems are common in children with ADHD. The next step is figuring out why sleep is off, then matching the fix to the cause. The research points the same way: start with sleep routines, and use melatonin as backup when it’s clearly needed.
Melatonin does have a place. It can shorten the time it takes a child to fall asleep, especially when a delayed body clock is part of the issue. But it has clear limits. It does not meaningfully improve inattention or hyperactivity, and long-term safety data in children is still limited. In one finding, stopping melatonin after long-term use led to a phase delay of sleep in 92% of children.
When routines don’t work, the next move isn’t “more melatonin.” It’s asking what’s actually driving the delay. In many cases, the issue goes past bedtime habits. Things like medication timing, anxiety, and circadian delay can all play a part. A clinician can help sort that out.
Key Points for Parents to Take Away
Melatonin works best when it supports steady sleep habits, not when it replaces them. The aim isn’t to stick with one tool no matter what. It’s to use the right support for the child’s sleep pattern. If sleep still hasn’t improved after several weeks of steady routines, bring in a clinician before increasing the dose or using melatonin for longer.
Frequently Asked Questions (FAQs)
How do I know if my child has a delayed body clock or poor bedtime habits?
It can be tough to tell the difference because both make falling asleep a struggle. A delayed body clock is biological; it naturally shifts your child’s sleep and wake times much later than usual. Poor sleep hygiene, however, is behavioral. Common routine problems include inconsistent schedules, screen time before bed, and too little daytime exercise. A professional evaluation is the best way to pinpoint the exact cause.
What should I do if sleep routines help a little but bedtime is still too late?
If behavioral sleep routines help only a little, the next step is to consult with a qualified healthcare professional or a dedicated sleep specialist. They can screen for hidden factors getting in the way of rest. Since children with ADHD frequently have a delayed circadian rhythm, a provider may recommend introducing melatonin as a clinical add-on option. Research shows that pairing structured sleep hygiene with low-dose melatonin is a highly effective approach for initial insomnia in this group.
When should I talk to a clinician before trying melatonin?
Talk to a clinician before starting melatonin if your child’s sleep problems are persistent, severe, or tied to other health issues.
The long-term effects in children still aren’t fully understood. A clinician can help you figure out whether melatonin makes sense, check for root causes behind the sleep disruption, and guide safe use, whether that means starting, continuing, or stopping it.
Is melatonin safe for toddlers and very young children with ADHD?
While short-term use is generally well-tolerated across pediatric age groups, you should never introduce melatonin to toddlers or young children without direct clinical supervision. A professional must first evaluate if the sleep disruption is linked to behavioral pushback, environmental factors, or stimulant medication timing before introducing any hormonal supplements.
What is the recommended melatonin dosage for children with ADHD?
There is no universal dosage because a child’s ideal response depends on their individual circadian rhythm rather than their age or weight. Clinical guidelines often favor lower doses (such as 0.5 mg to 2 mg) given 30 to 60 minutes before the desired bedtime, rather than massive doses taken right at lights-out. Seeking customized guidance from your clinical team ensures you utilize the smallest, most effective dose.
Comprehensive ADHD and Sleep Care at Modyfi Health
If your family is exhausted from nightly bedtime battles, you do not have to guess your way through sleep solutions alone. At Modyfi Health, our multidisciplinary team brings together board-certified psychiatrists, clinical nutritionists, and therapists to evaluate every angle of your child’s health.
We look beyond standard checklists to analyze the complete picture—coordinating lifestyle adjustments, behavior therapies, precise medication timing, and targeted metabolic testing. This collaborative approach ensures your child gets a seamless, integrated treatment plan designed to improve both nighttime rest and daytime focus.
✔️ Find a Modyfi Provider to Transform Your Family’s Sleep Today
{kind=link}