
Ecotherapy can support mood, stress, sleep, and treatment follow-through — but it works best alongside psychiatric care, not instead of it.
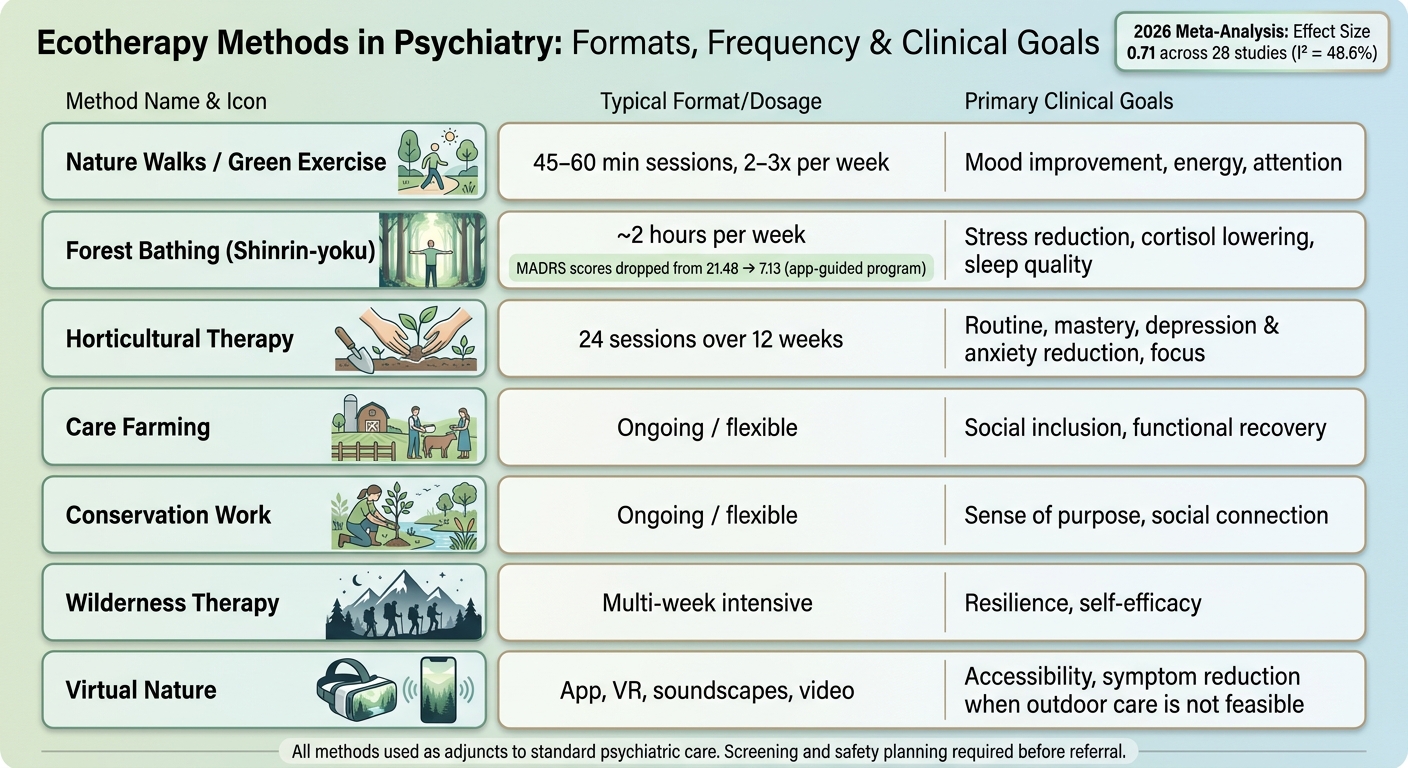
The research shows real promise. A 2026 meta-analysis of 28 studies found a pooled effect size of 0.71 for nature-based interventions on clinical psychiatric symptoms. In one forest therapy study, MADRS depression scores dropped from 21.48 to 7.13. These are meaningful numbers — with important caveats about study quality and duration that are worth understanding before drawing conclusions.
What the evidence actually shows:
- What it is: planned nature-based care used as part of psychiatric treatment.
- Formats include: walks, forest bathing, gardening, care farming, conservation work, wilderness programs, and virtual nature tools.
- Where it may help: depression, stress, sleep, attention, routine, and social connection.
- Important limit: it does not replace medication, therapy, crisis care, or psychiatric evaluation.
- Who may need a different setting: people with acute suicidality, active psychosis or mania, high elopement risk, or trauma tied to outdoor places.
- How clinicians use it: by matching the format to the person, setting goals, tracking symptoms with PHQ-9, GAD-7, MADRS, and PSQI, and confirming safety first.
Nature can be part of treatment — but the plan still needs structure, screening, and symptom tracking.
The table below summarizes the main formats used in clinical settings, along with typical frequency, duration, and primary therapeutic goals. Not every format fits every patient — the right match depends on diagnosis, mobility, safety, and personal preference.
| Method | Usual Format | Main Use |
|---|---|---|
| Nature walks / green exercise | 45–60 minutes, 2–3 times per week | Mood, energy, attention |
| Forest bathing | About 2 hours per week | Stress, sleep, cortisol |
| Horticultural therapy | 24 sessions over 12 weeks | Routine, depression, anxiety, focus |
| Care farming / conservation work | Flexible | Social contact, purpose, daily function |
| Wilderness therapy | Multi-week | Resilience, self-belief |
| Virtual nature | App, VR, audio, video | Access when outdoor care is hard |
Bottom line: ecotherapy has promise, but the evidence is still limited by short study lengths, mixed methods, and uneven reporting. So the best use is simple: add it to standard psychiatric care when the person, setting, and safety plan line up.
Ecotherapy: How Nature-Based Therapy Supports Mental Health with Dr. Amy Balentine
sbb-itb-23f89d4
Ecotherapy Methods Used in Mental Health Settings
Ecotherapy Methods in Psychiatry: Formats, Frequency & Clinical Goals
Nature Walks, Green Exercise, and Forest Bathing
Among the three, this group is the easiest ecotherapy method to use in practice. A typical session runs 45–60 minutes, two to three times per week.
Green exercise builds on that by adding planned movement, like walking, cycling, or light outdoor activity, in a natural setting. Research suggests outdoor exercise may offer psychological benefits — including reduced stress and improved mood — compared to indoor exercise, though the evidence quality varies across studies and effects aren’t universal.
Forest bathing (Shinrin-yoku) takes a different approach. It focuses on slow, sensory-based time in nature instead of effort or fitness. Sessions often last about two hours per week, and research links forest bathing to lower cortisol levels, better sleep quality, and stronger immune markers. That makes it a good fit for patients with limited mobility or low exercise tolerance.
Across all three approaches, structure and safety matter. Clinicians need to think through terrain, weather, and transportation before suggesting any outdoor program. Guided sessions led by trained facilitators tend to be more structured and more useful in clinical care than unguided exposure. Nature exposure lowers negative mood, and when mindfulness is added, positive mood improves as well.
Horticultural Therapy, Care Farming, and Conservation Work
These methods center on active involvement with living systems. Horticultural therapy uses gardening, planting, and food-growing tasks as planned therapeutic activities. A typical program includes 24 sessions over 12 weeks, and the evidence is strong for improving attention and reducing symptoms of depression and anxiety.
Care farming takes this work into farm settings, where patients join farm-based routines with staff and other participants. Conservation work, such as tree planting, habitat restoration, and trail maintenance, adds a sense of purpose that many patients respond to well in treatment. Care farming can help with social connection and day-to-day function, while conservation work strengthens purpose and social contact.
Some horticultural therapy programs also give patients access to fresh food, which can support nutrition goals as part of a broader treatment plan.
Wilderness Programs and Virtual Nature Interventions
Access, mobility, and weather often shape whether outdoor, intensive, or virtual care makes the most sense.
Wilderness and adventure therapy programs are the most intensive ecotherapy format. These are usually multi-week or expedition-based programs that use outdoor challenges, such as navigation, bush skills, and group problem-solving, to build psychological resilience and self-efficacy. They are not right for every patient. Before referral, clinicians need careful screening for physical health, psychiatric stability, and safety risk.
For patients who can’t get outdoors because of mobility limits, geography, or extreme weather, virtual nature interventions offer a practical option. These can include guided nature imagery, nature soundscapes, and video- or VR-based green environments. Virtual formats can reduce stress and improve access for patients who can’t use outdoor care. One smartphone-app-guided forest therapy program led to a drop in MADRS depression scores from 21.48 to 7.13.
The table below sums up the main format and clinical aim for each modality:
| Modality | Typical Format | Primary Clinical Goals |
|---|---|---|
| Forest Bathing | 2 hrs/week | Stress reduction, cortisol lowering, sleep |
| Green Exercise / Nature Walks | 45–60 min, 2–3x/week | Mood, vitality, attention |
| Horticultural Therapy | 24 sessions / 12 weeks | Routine, mastery, depression, anxiety |
| Care Farming | Ongoing / flexible | Social inclusion, functional recovery |
| Conservation Work | Ongoing / flexible | Purpose, connection, social contact |
| Wilderness Therapy | Multi-week intensive | Resilience, self-efficacy |
| Virtual Nature | App, VR, soundscapes | Accessibility, symptom reduction |
These formats vary in intensity, and each tends to work best when matched to a patient’s symptoms, safety needs, and access.
How Clinicians Combine Ecotherapy With Standard Psychiatric Treatment
After picking a format, clinicians weave ecotherapy into the rest of care: medication, psychotherapy, sleep, and nutrition. The goal is simple. Match the approach to safety concerns, symptom targets, and the treatment plan already in place.
Medication Management and Safety Monitoring Outdoors
Ecotherapy can sit alongside medication management as an adjunct, not a stand-alone treatment. That means clinicians still need to do the usual risk check before moving sessions outside.
They screen for heat, sun exposure, dehydration, photosensitivity, dizziness, fall risk, mobility limits, allergens, insects, and wildlife. If a patient has more risk factors, it often makes sense to start in managed green spaces or urban parks instead of less controlled native ecosystems.
Nutrition, Sleep, and Circadian Rhythm Support
Once safety is covered, timing becomes the next piece. Clinicians look at when to schedule sessions and how those sessions can support a steadier daily rhythm.
Morning walks and forest therapy may help anchor circadian rhythm and improve sleep quality. In one study, Pittsburgh Sleep Quality Index scores improved from a mean of 19.78 to 14.48 after a forest therapy program. Horticultural therapy and care farming may also help support regular meals and a steadier daily routine.
Psychotherapy Integration and Multidisciplinary Care
Ecotherapy isn’t limited to outdoor sessions. Therapists can bring ecotherapy ideas into standard psychotherapy even without a formal outdoor program. In practice, the outdoors can help with behavioral analysis, rapport, metaphor, narrative work, and stabilization.
Because ecotherapy cuts across more than one area of care, coordination matters just as much as the setting itself. Multidisciplinary teams can make nature-based rehabilitation feel more connected from a clinical standpoint.
Benefits, Evidence, and Clinical Limits
After the methods and care model, the next issue is simple: How well does ecotherapy work, and where are its limits?
What Research Shows About Mood, Stress, and Function
The early picture is encouraging. A 2026 meta-analysis of 28 studies found that nature-based interventions led to greater improvement in clinical psychiatric symptoms than controlled comparators, with a pooled effect size of 0.71. Other studies also point to gains in sleep, attention, somatic symptoms, and social connection.
A separate second-order meta-analysis published in Nature Human Behaviour — covering 116 systematic reviews and over 10 million participants — found significant reductions in anxiety (SMD = −0.83) and depression (SMD = −0.72) with nature-based interventions.
That said, good early results don’t erase the need for caution. It still matters to spell out where the research is strong, where it is thin, and which patients are a good match.
Limits of the Evidence and What Ecotherapy Cannot Do
The evidence is still incomplete. Across studies, research heterogeneity is moderate (I² = 48.6%), sample sizes vary a lot – from 8 to 781 participants – and most trials last fewer than 12 weeks. For anxiety disorders, findings are mixed, which makes direct comparison with conventional psychotherapy hard.
That matters in practice. Ecotherapy should be used as an adjunct to standard psychiatric care, not as a substitute for psychiatric evaluation, medication management, or urgent care.
The tradeoff is worth naming directly: the field shows promise, but the research base is not settled yet.
| Potential Benefits of Ecotherapy | Current Evidence Limits |
|---|---|
| Significant reduction in stress and cortisol levels | Small sample sizes in many pilot studies (n = 8 to 781) |
| Enhanced cognitive function (attention/working memory) | Lack of long-term follow-up data (most studies <12 weeks) |
| Improved sleep quality | Inconsistent intervention protocols and dosages |
| Potential for publication bias (under-reporting negative results) | |
| Poor reporting of participant demographics and specific diagnoses |
Contraindications and When Office or Virtual Care Fits Better
This is where clinical judgment comes in. Acute suicidality, active psychosis or mania that needs close supervision, severe functional impairment, and high elopement risk all call for a controlled clinical setting. In those cases, outdoor care is not the right fit.
Office or virtual care may also make more sense when outdoor conditions or medical risk make in-person sessions unsafe. The same goes for patients whose trauma history is directly tied to outdoor settings.
Those limits shape treatment planning, session format, and the level of monitoring needed.
Clinical Use, Treatment Planning, and Key Takeaways
How to Add Ecotherapy to a Psychiatric Treatment Plan
Once the approach and its limits are clear, the next step is turning it into an actual treatment plan. Start by looking at the patient’s diagnosis, current stability, mobility, and personal preference. Then match the type of ecotherapy to the goal. Horticulture can support purpose and attention, forest bathing can help with stress and sleep, and community gardening may help with social isolation.
Write the plan down in plain terms. Spell out the frequency, duration, activity, and outcome measures. For example, that might mean 30-minute park walks twice a week or six weekly two-hour forest therapy sessions. From there, track progress with standard tools such as PHQ-9 or MADRS for depression, GAD-7 for anxiety, and PSQI for sleep.
Safety matters here. Think through allergens, weather, terrain, tick- or mosquito-borne illness risk, restroom access, and informed consent. It also helps to bring in the right team. Psychiatrists, therapists, occupational therapists, and trained nature facilitators can work together to keep the plan safe and coordinated.
If getting outside isn’t realistic, don’t force it. Virtual nature exposure or guided outdoor homework between sessions can still fit the plan. That makes ecotherapy easier to use in day-to-day clinical care.
Key Takeaways
Use ecotherapy as an adjunct to standard care. The evidence is encouraging, but it’s still limited. The best candidates are patients whose goals line up with a nature-based intervention. If outdoor treatment is unsafe or impractical, stick with office-based or virtual care.
Ecotherapy works best as an adjunct, not a standalone treatment. Use it when the setting, safety, and patient goals line up.
Ready to Build a Care Plan That Works With Your Whole Life?
Ecotherapy is one piece of an integrative approach to mental health — and when it fits, it works best alongside psychiatric care, therapy, nutrition, and movement, not in isolation. At Modyfi, our Root-Cause Psychiatry model brings all four together, so nature-based care can be part of a plan that’s actually built around you.
👉 Explore Providers to Book an Appointment and Start Your Care Plan
(Note: Modyfi proudly accepts most major commercial insurance plans in MD, DC, VA, and WV; currently, we do not accept Medicare or Medicaid.)
FAQs
Who is a good candidate for ecotherapy?
Ecotherapy is a flexible, complementary approach that can support mental health and overall well-being. It may be a good fit for people dealing with anxiety, depression, stress-related conditions, and mood imbalances.
It can also help people living with PTSD, adjustment disorders, and somatoform disorders. And because ecotherapy can be as simple as a walk in the park or as structured as a guided group program, it may work well for adolescents, young adults, and adults living in the community.
Can ecotherapy replace medication or therapy?
Ecotherapy is not a direct substitute for medication or standard psychotherapy. It tends to work best as one part of a broader psychiatric care plan.
Research suggests it may bring short-term relief for depression at a level similar to cognitive behavioral therapy. But it works best when it’s used alongside structured, evidence-based medical and mental health care.
What if outdoor treatment is not safe or practical?
When outdoor treatment isn’t safe or practical, clinicians put patient safety and therapeutic stability first. In those cases, care can move to office-based or virtual settings, where the environment is more controlled and predictable for psychotherapy and clinical care.
Is ecotherapy covered by insurance?
It depends — and the honest answer is that coverage for ecotherapy specifically is limited in most insurance plans. Because ecotherapy is still emerging as a formal clinical modality, most insurers don’t have a dedicated billing code for it. That means it’s rarely reimbursed as a standalone service.
That said, when ecotherapy is delivered as part of a broader psychiatric or therapeutic treatment plan — by a licensed clinician, documented as a component of care — it may be covered under existing mental health benefits. The key is how it’s framed and documented in the treatment record.
In practice, this means the most practical path to insurance coverage is through an integrated care setting where a licensed provider incorporates nature-based approaches into a broader, medically documented plan. Working with a clinician who understands both the clinical evidence and the documentation requirements makes a meaningful difference in what gets covered.
If you’re unsure what your plan covers, the most reliable first step is calling the member services number on your insurance card and asking specifically about outpatient mental health benefits and what documentation is required for reimbursement.
{kind=link}