
{kind=link}
Virtual psychiatric support offers an effective, validated lifeline for older adults navigating mental health changes. Robust clinical data confirms that remote mental health care delivers symptom improvement and patient satisfaction rates that closely mirror traditional, face-to-face clinic visits. For seniors residing in rural areas, those who are homebound, or individuals living in long-term care communities, this approach removes the exhausting friction of medical transit without sacrificing clinical excellence.
The Baseline Verdict:
Clinical evidence confirms that telepsychiatry serves as an outstanding, validated resource for older adults navigating depression, anxiety, routine follow-up consultations, and caregiver-supported dementia care. Rather than treating online treatment as a universal solution, recognizing its specific clinical boundaries ensures that care parameters are always safely matched to each senior’s individual physical and cognitive profile.
When we evaluate the deep clinical research surrounding geriatric telepsychiatry effectiveness, several structural milestones stand out:
-
Targeted Symptom Reduction: Controlled research shows that video-based assessments match in-person evaluations across mood, anxiety, and general psychiatric disorders. A rigorous clinical review evaluating 1,663 older adults demonstrated a marked reduction in depressive symptoms, noting that the most significant drop occurs within the first 3 months of treatment.
-
High Operational Satisfaction: Patient and caregiver acceptance metrics remain high and closely parallel traditional clinic settings. For instance, a landmark outpatient study recorded a virtual care satisfaction score of 4.1 out of 5, compared to 4.2 out of 5 for in-person visits, proving that digital delivery preserves trust.
-
Dignified Access Expansion: The most substantial functional gains show up among seniors who experience physical vulnerabilities or geographical constraints. By eliminating the logistical trauma of clinic travel, integrated virtual networks successfully bridge care disparities for underserved populations.
-
Proactive Boundary Management: Embracing transparency means acknowledging that virtual formats require deliberate, thoughtful environmental tailoring. Sensory shifts—such as uncompensated hearing loss, vision challenges, or complex cognitive changes—can occasionally cloud standard video screen dynamics.
To smooth out these digital speedbumps, implementing structured workflows like pre-visit technology dry-runs, enlarged large-print instructional materials, and active caregiver setup support safely preserves clinical accuracy and rapport on screen.
To synthesize the vast clinical literature surrounding geriatric telepsychiatry effectiveness, the baseline data matrix below maps specific diagnostic categories against proven real-world outcomes:
| Area | What the research says |
|---|---|
| Symptom outcomes | Often similar to in-person care |
| Depression | Best-studied condition |
| Anxiety | Good early support |
| Dementia care | Caregiver outcomes often improve |
| Access | Often better for rural, homebound, and long-term care patients |
| Satisfaction | Usually high |
| Main barriers | Internet access, sensory limits, cognitive issues, privacy, policy rules |
The visual overview below maps the core boundaries of geriatric telepsychiatry effectiveness, highlights diagnosis-specific clinical outcomes, and identifies where specialized environmental adjustments remain essential for care delivery:
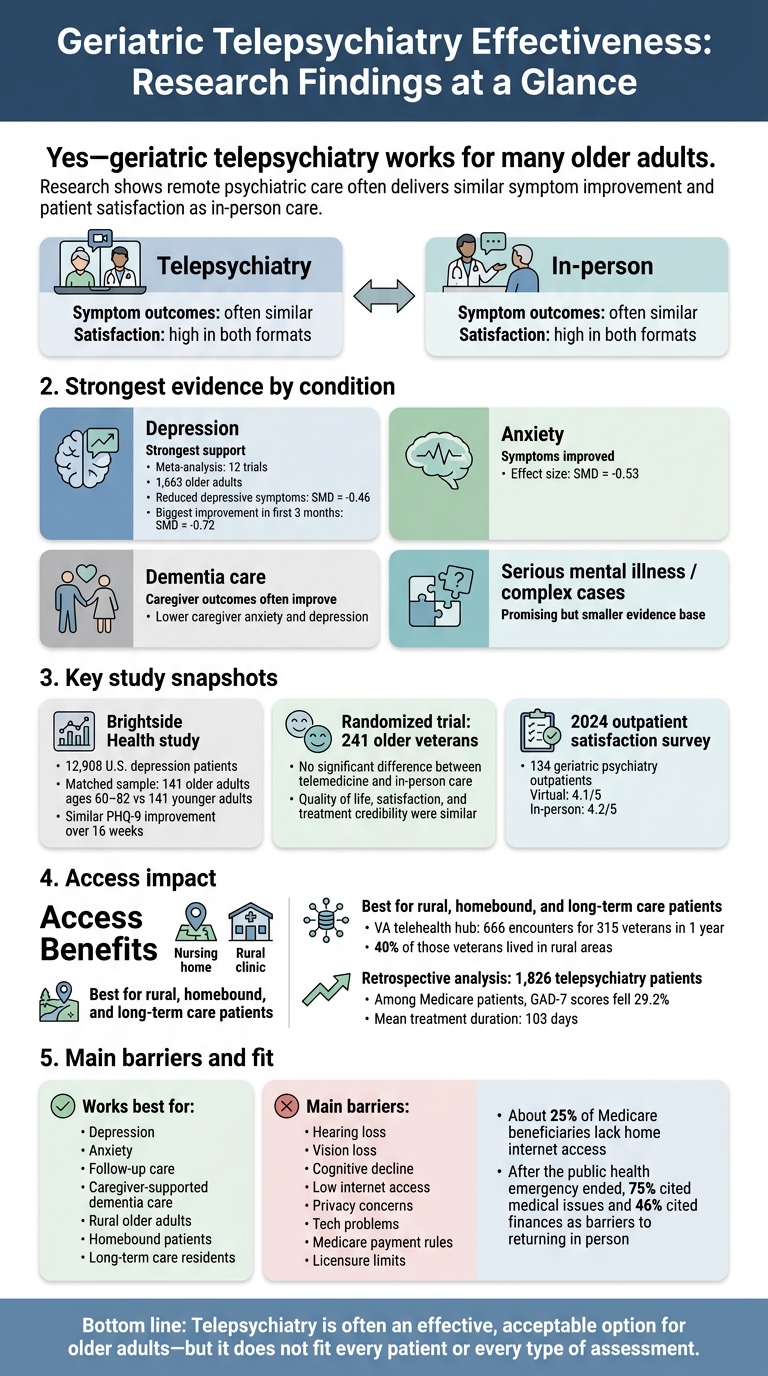
Geriatric Telepsychiatry Effectiveness: Research Findings at a Glance
Development of Telehealth Principles and Guidelines for Older Adults: A Modified Delphi Approach
sbb-itb-23f89d4
What the Research Shows About Effectiveness
Peer-reviewed studies show that telepsychiatry for older adults can match in-person care for symptom relief and quality of life. It can also improve no-show rates and wait times. The big issue is simple: can remote care help close access gaps without cutting the quality of care?
Diagnostic Reliability of Video-Based Psychiatric Assessment
For many cases, video-based psychiatric interviews line up closely with in-person evaluations. That includes mood disorders, anxiety, and broad psychiatric assessments in older adults. In rural telegeriatric clinics, remote visits led to more new diagnoses (p = 0.002) and more medication changes (p = 0.009) than in-person visits.
That said, video is not a perfect fit for every kind of assessment. Cognitive screening and more complex neuropsychiatric evaluations need extra care. Hearing loss, vision loss, and advanced cognitive impairment can make video-based assessment less reliable.
Diagnostic accuracy matters, of course. But the bigger test is whether people actually feel better after treatment.
Clinical Outcomes Compared With In-Person Care
A Brightside Health study of 12,908 U.S. patients receiving depression care found similar outcomes in older and younger adults. Researchers used propensity matching to compare 141 older adults ages 60–82 with 141 younger adults. Both groups showed significant and similar decreases in PHQ-9 scores over 16 weeks. The researchers concluded that older adults improved at a similar rate over 16 weeks, which suggests age did not limit benefit from telepsychiatric care.
A second randomized trial pointed in the same direction. In a separate randomized trial of 241 older veterans, researchers found no significant difference between telemedicine and in-person care for quality of life (SF-36 scores), patient satisfaction, or treatment credibility.
The strongest results show up in symptom improvement and access. Even so, findings can differ by condition, and later results show some diagnosis-specific variation. Depression has the clearest support, while other diagnoses need a closer look.
Findings by Mental Health Condition
Depression, Anxiety, and Late-Life Depression
Depression has the strongest evidence among specific conditions in geriatric telepsychiatry.
A meta-analysis of 12 randomized controlled trials covering 1,663 older adults found that telecare reduced depressive symptoms compared with usual care (SMD = -0.46). The biggest drop showed up in the first 3 months of treatment (SMD = -0.72).
Anxiety improved at a similar level (SMD = -0.53).
Dementia, Behavioral Symptoms, and Caregiver Outcomes
In dementia care, the steadiest gains show up in caregiver outcomes.
Home-based video care improved outcomes for both patients and caregivers, including lower caregiver anxiety and depression. Group therapy delivered through the same format also helped caregivers. Reports showed shorter hospital stays, lower dropout, better therapy engagement, and symptom reduction.
Serious Mental Illness and Complex Medical Comorbidity
Here, the evidence comes mostly from specialty programs and pilot studies rather than large trials.
One example is the Senior Care Action Network (SCAN) Group in Southern California. It ran a primary care-based telepsychiatry program for 218 older adults from February 2019 to August 2020. Many participants had prior psychiatric hospitalizations, substance use disorders, or several chronic medical conditions. After the first telepsychiatry visit, outpatient use dropped by 0.24 per patient, emergency department visits dropped by 0.07 per patient, and hospitalizations dropped by 0.03 per patient during each 6-month period.
That’s encouraging, especially for high-risk seniors. At the same time, the evidence base is still small.
These clinical results set up the next issue: whether patients, caregivers, and clinicians accept virtual care.
Satisfaction, Access, and Barriers in Practice
Clinical benefit only goes so far if older adults won’t use the service. That’s why satisfaction matters. When people feel good about the experience, they’re more likely to stick with care, which helps maintain the clinical gains described above.
Patient, Caregiver, and Clinician Satisfaction
Satisfaction is high and comes close to in-person care. A 2024 survey of 134 geriatric psychiatry outpatients at Zucker Hillside Hospital in Glen Oaks, NY found that virtual care satisfaction averaged 4.1 out of 5, compared with 4.2 out of 5 for in-person visits. After the public health emergency ended in May 2023, 75% cited medical issues and 46% cited finances as barriers to returning in person.
Clinicians also point to better access, more flexibility, lower costs, and improved efficiency.
Still, the downsides are real. Privacy at home can be hard to protect. Tech problems can interrupt the visit. And video calls can make it tougher to pick up on face-to-face cues.
Here’s how those tradeoffs tend to show up across groups:
- Patients often like the convenience and the chance to get care from home, but privacy concerns, sensory loss, and discomfort with technology can get in the way.
- Caregivers can join visits more easily, though they often end up helping with setup.
- Clinicians tend to like the flexibility and efficiency, while long-term care staff benefit from faster access to specialists.
Access Gains for Rural, Homebound, and Long-Term Care Populations
The biggest gains show up among patients who have a hard time traveling. Put simply, telepsychiatry removes the trip to the clinic. For homebound older adults and those dealing with mobility limits, chronic illness, or transportation gaps, that can make the difference between getting care and going without it.
A Veterans Health Administration regional telehealth hub evaluation found that a single board-certified geriatric psychiatrist conducted 666 encounters for 315 veterans in one year, with 40% of those veterans living in rural areas. A separate retrospective analysis of 1,826 patients receiving telepsychiatric care between February and September 2023 found similar improvements in anxiety and depression scores across rural and urban patients. Among Medicare patients, GAD-7 scores fell 29.2% over a mean treatment duration of 103 days.
“The finding that treatment efficacy was comparable among rural and urban patients indicated that telepsychiatry is a promising approach to overcome treatment disparities that stem from geographical constraints.” – Cheryl Person, MD, MBA
In long-term care settings, telepsychiatry is feasible and well accepted for consultations, cognitive testing, and dementia management.
Digital Literacy, Sensory Impairments, and Policy Constraints
Access gains don’t reach everyone in the same way. About 25% of Medicare beneficiaries lack home internet access. That gap hits older adults from minority backgrounds and those enrolled in Medicaid harder, since both groups are statistically less likely to use video visits.
Sensory and cognitive issues can also make virtual care harder to use. Hearing loss, vision impairment, hand tremors, and cognitive decline can all create friction. Studies point to a few practical fixes: pre-visit tech rehearsals, paper copies of simplified large-print instructions, adaptive equipment matched to each patient’s sensory needs, and staff help during connection setup. Clinicians have also found that slowing speech, using simple analogies, and staying patient during tech problems can help preserve rapport on screen.
Policy is another sticking point. Medicare payment rules and licensure limits still slow broader adoption. Long-term use still depends on equal Medicare payment and simpler licensure rules.
Integrated Virtual Care Models and Key Takeaways
Multidisciplinary Models in Virtual Geriatric Mental Health
Clinical data confirms that virtual mental health support falls short when treated as an isolated video call—it thrives when it operates as an interconnected ecosystem. Sustainable recovery happens when specialized clinicians actively cross-pollinate ideas rather than working in silos.
At Modyfi, we bridge this gap by seamlessly locking precision psychiatry, targeted talk therapy, functional nutrition, and restorative exercise into a singular, unified network of providers. Simultaneously addressing metabolic, physical, and cognitive health ensures that treating late-life anxiety or depression moves beyond a temporary band-aid into deep biological revitalization
We see excellent structural validation for this in institutional networks, such as the Veterans Health Administration’s regional hub-and-spoke frameworks. By utilizing remote consultations, a single specialized geriatric psychiatrist can stabilize multiple underserved communities at once.
On the ground, these collaborative ecosystems maximize clinical outcomes because operational roles are beautifully distinct:
- Specialized Psychiatrists deliver precise evaluations, diagnostic clarity, and intentional medication management.
- Primary Care Clinicians interface directly with the patient to smoothly execute and monitor the baseline care blueprint.
- Caregivers and On-Site Staff anchor the daily environment, assisting with digital logistics, tracking patient history, and providing vital behavioral support.
Bringing psychiatry, behavioral therapy, nutrition, and lifestyle coordination into a single loop fundamentally removes the confusing fragmentation that historically derails senior healthcare.
Evidence Gaps and Final Summary
Evaluating clinical data with integrity requires identifying where research currently falls short. While geriatric telepsychiatry effectiveness is deeply validated for mainstream mood conditions, historical literature exhibits a clear demographic slant.
Most available trials lean heavily toward tech-literate populations and lack diverse racial representation. Furthermore, clear clinical data remains limited for adults over the age of 80, individuals navigating advanced stages of dementia, and those with severe, uncompensated sensory loss.
Despite these systemic research boundaries, the macro data delivers an incredibly clear verdict: virtual mental health care is deeply effective and highly accepted by older adults.
The clinical equity advantages break down into three primary high-impact profiles:
- Geographically Isolated Seniors: Removing the physical burden of travel instantly bridges rural care disparities.
- Homebound Individuals: Patients managing severe chronic physical illnesses gain reliable, consistent access to specialists.
- Long-Term Care Residents: Assisted living facilities achieve rapid, fluid consultations without the logistical trauma of external medical transport.
Ultimately, digital psychiatry shifts from a novel convenience into a definitive clinical asset when workflows are engineered around human reality. Success relies entirely on smooth ecosystem execution. When professional clinician networks, proactive on-site support, and transparent medical design are seamlessly looped together, virtual care unlocks a clear, dignified pathway toward lasting mental vitality.
FAQs
Is telepsychiatry as effective as in-person care for seniors?
Yes. Peer-reviewed clinical literature demonstrates that telepsychiatry achieves diagnostic reliability and symptom reduction outcomes that directly match traditional, face-to-face geriatric care.
Controlled trials reveal no statistically significant variance in client satisfaction, quality of life metrics, or the acceleration of depression treatment success. While digital logistics can occasionally present a brief initial learning curve, clinical data proves that age itself is never a barrier to sustainable recovery.
Which older adults benefit most from geriatric telepsychiatry?
Geriatric telepsychiatry can make a big difference for older adults who have a hard time getting in-person psychiatric care, especially people living in rural or underserved areas.
Research also points to strong results for seniors dealing with moderate to severe depression, anxiety, co-occurring substance use disorders, and multiple physical health conditions. It can also help people in long-term care who need support for neuropsychiatric symptoms.
Does insurance cover virtual geriatric psychiatry?
Yes, commercial insurance coverage for virtual psychiatric care is widely available, though specific parameters vary by network. Modyfi actively prioritizes medical accessibility by accepting most major commercial insurance plans in Maryland, Washington D.C., Virginia, and West Virginia.
By directly managing the complexities of insurance verification on your behalf, we protect your focus from administrative friction. Please note: Our specialized network does not currently interface with Medicare or Medicaid platforms.
When is telepsychiatry not the best fit for seniors?
Telepsychiatry works well for many seniors. But it isn’t the right fit for every person.
For some older adults, physical or cognitive challenges can make video visits harder to use. Others may not have steady internet access, the right device, or much comfort with digital tools. That can turn a simple appointment into a frustrating experience.
At Modyfi Health, we look at those needs upfront so we can match care to each patient’s abilities and day-to-day situation.
How does Modyfi’s senior mental health care model differ from a standard video call?
We do not treat virtual care as an isolated, transactional video appointment. Standard therapy models often look at mental health in isolation, but Modyfi treats the individual as a complete biological ecosystem. We loop precision psychiatry, targeted therapy, functional nutrition, and tailored exercise into one integrated network of providers.
This allows us to investigate underlying biological root causes—such as gut health, systemic inflammation, or nutritional gaps—ensuring a comprehensive baseline for cognitive wellness and vibrant daily performance.
Caring for your own mental health—or coordinating care for an aging loved one—requires a deep understanding of how the brain, body, and daily lifestyle habits interface. Modyfi Health dismantles fragmented healthcare by gathering precision psychiatry, dedicated therapy, functional nutrition, and restorative exercise under one virtual roof. Our specialized network of providers works as your guided strategic resource, treating you as an ecosystem to be balanced rather than a diagnosis to be managed.
👉 Explore Providers to Book an Appointment and Start Your Care Plan
Want to meet our network first before diving in? You can also Book a FREE 15-Minute Discovery Call with our care guides.
(Note: Modyfi proudly accepts most major commercial insurance plans in MD, DC, VA, and WV)