
Omega-3s are one of the most researched supplements for ADHD — but the results depend heavily on the type and dose used. The main pattern in research is this: EPA-heavy fish oil, often with more than 500 mg of EPA per day and a 2:1 EPA-to-DHA ratio, shows the most consistent signal, while many studies show little or no change.
What the evidence actually shows:
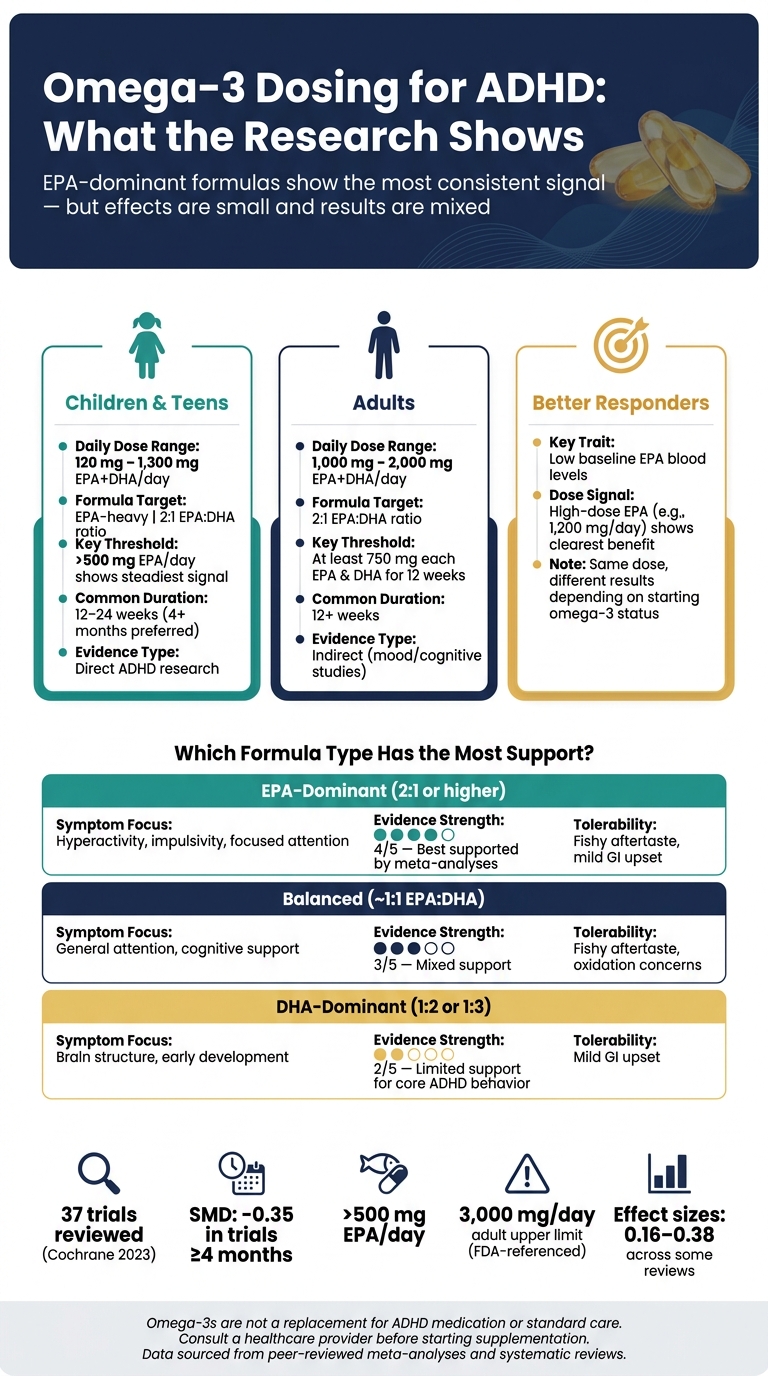
- Omega-3s support standard ADHD care — they don’t replace medication or therapy
- Evidence is mixed: some reviews show modest benefit, while a 2023 Cochrane review found little to no meaningful change
- EPA matters more than DHA, especially in doses above 500 mg/day with a 2:1 EPA-to-DHA ratio
- Dosing varies by age — children and teens have used 120–1,300 mg/day combined EPA+DHA; adult ADHD data is limited
- Time matters — benefits, if present, often take 4+ months to appear
- Side effects are mild (fishy aftertaste, stomach upset, occasional nosebleeds), but doses above 3,000 mg/day in adults need medical guidance.
What the Research Actually Shows About Omega-3 and ADHD
sbb-itb-23f89d4
Quick Comparison
Omega-3 Dosing for ADHD: EPA vs. DHA, Age Groups & Evidence Strength
| Group | Daily amount studied | Formula pattern | What research suggests |
|---|---|---|---|
| Children & teens | 120 to 1,300 mg/day | EPA-heavy, often 2:1 EPA:DHA | Small, uneven effects; better signal in some higher-EPA studies |
| Adults | 1,000 to 2,000 mg/day | Often around 2:1 EPA:DHA | Limited direct ADHD data; evidence is less clear |
| Higher-response group | Varies | Higher EPA share | People with low baseline omega-3 levels may respond better |
What I take from the article is simple: dose matters, but formula and starting omega-3 status may matter just as much. If someone is looking at omega-3s for ADHD, the research points more toward EPA-dominant daily dosing over several months, not low-dose or short-term use.
Note: Exact ratios vary by study, typically ranging from 2:1 to 2.5:1, with EPA as the dominant fatty acid.
What Studies Show: Small Benefits, Mixed Results, and Common Dose Patterns
What Meta-Analyses and Systematic Reviews Found
Some meta-analyses reported small gains in ADHD symptoms with omega-3 supplements. But the bigger picture is still mixed.
The 2023 Cochrane review looked at 37 trials and found little evidence of meaningful symptom change in children and adolescents. Parent-rated inattention (SMD: -0.01) and hyperactivity (SMD: 0.09) were basically unchanged over the study period.
So the plain-English takeaway is pretty simple: if omega-3s help, the effect tends to be small and uneven. One big reason is that the studies didn’t all test the same thing. Dose levels varied. Trial length varied too. That makes head-to-head comparison messy.
Why Study Results Differ: Duration, Outcomes, and Design
The inconsistency usually comes down to a few recurring issues:
First, study length matters. A 2023 meta-analysis of 22 studies found no significant overall improvement (SMD: -0.16), but trials lasting at least 4 months did show a significant benefit (SMD: -0.35, p=0.007). That points to a simple problem: short trials may end before any change has time to show up.
Second, blood omega-3 levels may take months to level off. If that’s the case, a brief study may not tell you much about what a steady daily dose can do over time.
Third, the way results are measured can shape what researchers see. Parent and teacher rating scales can be affected by placebo effects, and gains on those scales don’t always show up on objective tests. On top of that, if a child is already taking stimulants, there may be less room for omega-3s to add much on top of that.
That’s why one trial can look promising while another lands flat. Same supplement category, different setup.
Comparison Table: Study Type, Population, Dose Range, and Effect Size
The clearest pattern isn’t one best dose. It’s how much the study designs differ.
| Study / Review | Population | Daily EPA+DHA Range | Duration | Main Finding |
|---|---|---|---|---|
| Cochrane Review | Children & Teens | Variable | 2 weeks – 6 months | No effect on parent-rated overall ADHD symptoms |
| Liu et al. 2023 | Children & Teens | Variable | < 4 months vs. ≥ 4 months | Significant benefit only in trials ≥ 4 months (SMD: -0.35) |
| Bélanger et al. | Children (ages 6–12) | 20–25 mg/kg EPA | 16 weeks | Significant improvement in parent Conners’ scores* |
*Conners’ scores (a standard rating scale clinicians use to assess ADHD symptoms)
Daily Omega-3 Dose Ranges Studied in Children and Adults With ADHD
Children and Teens: Trial Dose Ranges and EPA-Heavy Formulas
Pediatric trials have tested combined EPA + DHA doses from as low as 120 mg/day up to 1,300 mg/day. Those numbers reflect what researchers used in ADHD studies, not general supplement advice.
Here’s the main takeaway: EPA-heavy formulas above 500 mg/day show the steadiest signal for hyperactivity and impulsivity. In youth, a combined dose of at least 750 mg/day of EPA + DHA is also a common cutoff mentioned in the research.
Some studies didn’t use one fixed daily dose. Instead, they based the amount on body weight. For example, the Bélanger et al. study gave children 20–25 mg/kg/day of EPA and 8.5–10.5 mg/kg/day of DHA, with a 2.5:1 EPA-to-DHA ratio. High-dose EPA at 1,200 mg/day has also shown benefit in children who started with low baseline EPA levels.
Adult ADHD trials are much fewer, and most of the dose data comes from nearby areas of research rather than direct ADHD studies.
Adults: Typical Trial Doses and Limits of the Evidence
Adult ADHD data are sparse. Most dose information comes from mood and cognitive studies, not direct ADHD trials. That means adult dosing guidance is less certain than pediatric dosing.
In those related studies – especially work on major depressive disorder – doses often land in the 1,000–2,000 mg/day combined EPA + DHA range, often with a 2:1 EPA-to-DHA ratio. An expert panel suggested at least 750 mg each of EPA and DHA daily for 12 weeks before judging response.
Even with that, adult ADHD dosing is still unclear, and current evidence does not support a firm clinical standard.
Comparison Table: Low-, Moderate-, and High-Dose ADHD Study Ranges
The pattern below shows how dose ranges differ by age group.
| Population | Total Daily EPA+DHA Range | EPA Emphasis | Main Outcomes | Evidence Type |
|---|---|---|---|---|
| Children & Teens | 120 mg – 1,300 mg | >500 mg EPA daily | Inattention, hyperactivity, impulsivity, vigilance | Direct ADHD research |
| Adults | 1,000 mg – 2,000 mg | 2:1 EPA-to-DHA ratio | Cognitive function, mood, inattention | Indirect support; not ADHD-specific |
Total milligrams matter less than the EPA share. The next section gets into why the EPA:DHA ratio may matter more.
Dose, EPA:DHA Ratio, Safety, and Individual Response
EPA vs. DHA: Why Formulation May Matter More Than Total Milligrams
After dose, the next issue is which fatty acid you’re getting. In many cases, the EPA:DHA ratio matters more than the big number printed on the front of the bottle. DHA helps with structure. EPA is the part more often tied to behavior-related changes in ADHD studies.
That helps explain why EPA-heavy formulas – especially products with an EPA-to-DHA ratio of 2:1 or higher – show up most often in trials linked to ADHD symptom change. One meta-analysis found that omega-3 supplements with more than 500 mg/day of EPA improved hyperactivity and impulsivity in particular. Clinical reviews also often point to a 2:1 EPA-to-DHA ratio as a common target for behavior support.
There’s also a simple label-reading issue here: check the Supplement Facts panel, not the front label. A product can advertise a big total milligram count while delivering much less actual EPA and DHA than you’d expect.
Side Effects, Safety, and Upper Intake Levels
Once you’ve picked a formula, day-to-day use comes down to side effects and dose limits. Omega-3s are usually well tolerated, but they’re not side-effect free. The issues reported most often are fishy aftertaste, mild indigestion, and nosebleeds.
If stomach upset becomes a problem, a few small changes can help:
- Take the supplement with a full meal
- Freeze capsules before swallowing
- Try a liquid emulsion instead
For adults, the FDA-referenced upper intake level is about 3,000 mg/day of combined EPA + DHA from supplements. Going past that without medical guidance isn’t advised. For children, dosing should follow pediatric guidance.
Bleeding risk is one area where extra care matters. People taking blood thinners, those with a clotting disorder, or anyone scheduled for surgery should talk with a healthcare provider before starting or staying on omega-3 supplements. The same goes for people with fish allergies or allergies to carrier oils used in some products, such as sunflower oil.
Quality matters too. Third-party testing seals like IFOS (International Fish Oil Standards), USP, or NSF can help confirm that a product has been checked for heavy metals such as mercury and lead, and that the oil has not gone rancid.
Comparison Table: EPA-Dominant vs. Balanced Formulas and Safety Considerations
| Formula Type | Typical EPA:DHA Ratio | Symptom Domain Studied | Strength of Evidence | Common Tolerability Issues |
|---|---|---|---|---|
| EPA-Dominant | 2:1 or higher | Hyperactivity, impulsivity, focused attention | Best supported – EPA >500 mg/day supported by meta-analyses | Fishy aftertaste, mild GI upset |
| Balanced | ~1:1 | General attention, cognitive support | Mixed support – broader but less specific improvements | Fishy aftertaste, oxidation concerns |
| DHA-Dominant | 1:2 or 1:3 | Brain structure, early development | Limited support for core ADHD behavior | Mild GI upset |
Response can still differ a lot from one person to another. One reason is baseline omega-3 status. Children who begin with low EPA blood levels tend to show the clearest improvements when given high-dose EPA. That helps explain why the same supplement can seem helpful for one child and do much less for another.
Clinical Context, Research Limits, and Key Takeaways
Why Personalization Matters When Choosing an Omega-3 Dose
A person’s starting point seems to matter a lot. Children with lower EPA and DHA blood levels at baseline tend to respond better. If those levels are already adequate, the effect is often much smaller.
Inflammation may matter too. Higher inflammation may predict a better response to EPA-heavy formulas. Age and body size can also shape results. On top of that, concurrent medications and genetic differences in fatty-acid metabolism may change how well someone responds.
That helps explain why study findings are so hard to line up side by side. Two kids can take the same product at the same dose and still get different results.
Medication interactions also matter. So even though omega-3 supplements are sold as natural products, they should not be treated as harmless by default.
Key Research Gaps to Keep in Mind
These mixed findings do not come from biology alone. A lot of the problem is in the way the studies are built. Many trials are small, short, and inconsistent, which makes it hard to pin down one best dose.
Two gaps stand out:
- Most trials do not measure starting omega-3 levels.
- Long-term safety data for higher doses in children remain limited.
Conclusion: What the Research Shows
Taken together, the research points to modest, not dramatic, effects. Omega-3s may help with ADHD in small and uneven ways, with somewhat better results from EPA-dominant formulas. But they fit best as an adjunct to standard treatment, not as a replacement for it. That standard treatment often includes behavioral therapy, medication management when appropriate, and attention to diet, sleep, and physical activity — the kind of whole-person approach that tends to get better results than any single supplement on its own.
Dose choice should be individualized and guided by a clinician who can check baseline status and watch for interactions.
FAQs
How long should omega-3s be taken before expecting ADHD benefits?
Research suggests omega-3s usually need daily use for at least 3 to 4 months before potential ADHD benefits may show up.
That timing makes sense. Omega-3s work by shifting the fatty acid makeup of cell membranes, and that takes time. Because of that, clinical guidance for kids and teens often points to 16 to 24 weeks of supplementation when the goal is to help with symptoms.
Should I choose a fish oil with more EPA than DHA for ADHD?
Yes. Research suggests the fatty acid ratio matters for ADHD, and more EPA than DHA tends to be the better fit.
Experts often suggest an EPA-to-DHA ratio of about 2:1, along with at least 500 mg of EPA per day. When you check a supplement label, look at the exact EPA and DHA amounts – not just the total fish oil listed on the front.
Who is most likely to benefit from omega-3s for ADHD?
People with ADHD who have a low omega-3 index or high inflammation may be the ones most likely to benefit from omega-3 supplements. Research also points in the same direction for younger patients: children and teens with ADHD often show lower blood levels of these fatty acids.
Can my child take omega-3s alongside ADHD medication like stimulants?
In most cases, yes — omega-3 supplements and stimulant medications work through different mechanisms, so there’s no inherent conflict between them. In fact, several studies on omega-3s for ADHD were conducted in children already taking stimulant medication.
That said, the research suggests something worth knowing: when a child is already on an effective stimulant dose, there may be less room for omega-3s to add a noticeable improvement on top of that. The supplement isn’t harmful in combination — it’s just that the effect may be harder to detect when the main symptoms are already well managed.
As with any addition to a treatment plan, it’s worth checking in with the prescribing clinician first, especially to review the full picture of what’s being used and why.
How do I know if my child has low omega-3 levels?
The only reliable way to know is through a blood test — specifically, one that measures the omega-3 index or individual fatty acid levels like EPA and DHA. Guessing based on diet alone isn’t accurate enough, since absorption and metabolism vary from person to person.
This matters because the research is fairly consistent on one point: children who start with lower baseline EPA levels tend to see more noticeable improvement from supplementation. Without knowing where a child’s levels stand, it’s hard to predict whether omega-3s are likely to help much at all.
This kind of baseline testing is something a clinician can order and interpret as part of a broader evaluation — rather than starting a supplement and hoping for the best.
Your Child’s ADHD Plan Shouldn’t Be One-Size-Fits-All
Whether you’re researching this for yourself or for your child, the research is clear on one thing: omega-3s work differently depending on baseline levels, symptoms, and what else is part of the care plan. Modyfi’s network of providers brings psychiatry, therapy, nutrition, and exercise together to build a plan around the person — not a generic dose.
{kind=link}